Background
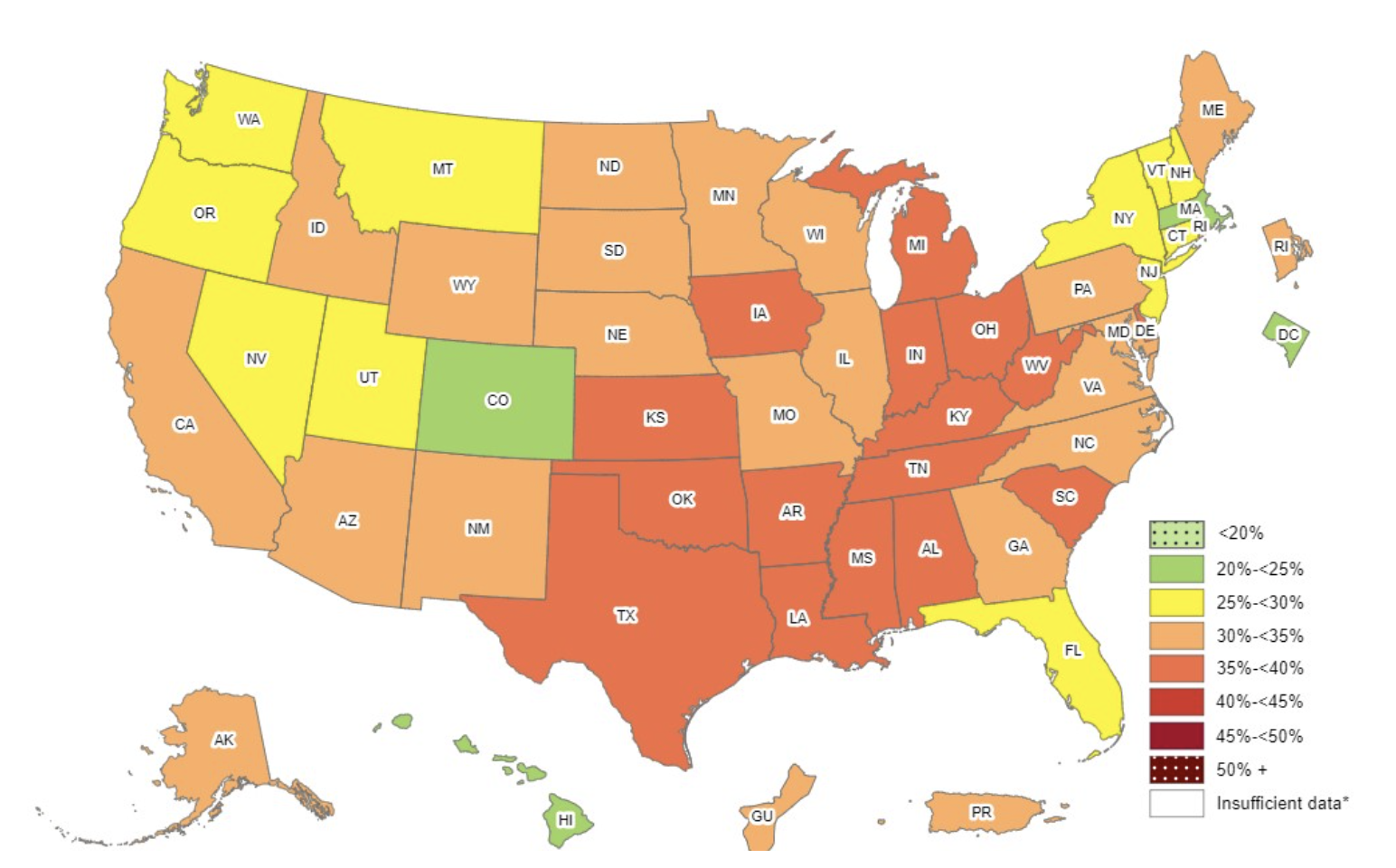
Obesity is a severe health concern across the world, and can contribute to other health problems including cardiovascular risk factors, high blood pressure, and social and psychological problems. Currently, more than 30% of U.S adults are obese and obesity rates are high among U.S children. According to the Division of Health and Nutrition Examination Surveys, obesity rates in U.S children and teenagers has more than tripled since the 1970s. The most recent Centers for Disease Control and Prevention (CDC) data shows that about 20% of U.S children are obese. Adolescents have a higher prevalence of obesity (22.2%) than children aged 2-5 years (12.7%). The childhood obesity rate is disproportional among race groups. Hispanic children are more likely to be obese (26.2%) than non-Hispanic Black children (24.8%), non-Hispanic White children (16.6%), and non-Hispanic Asian children (9.0%).
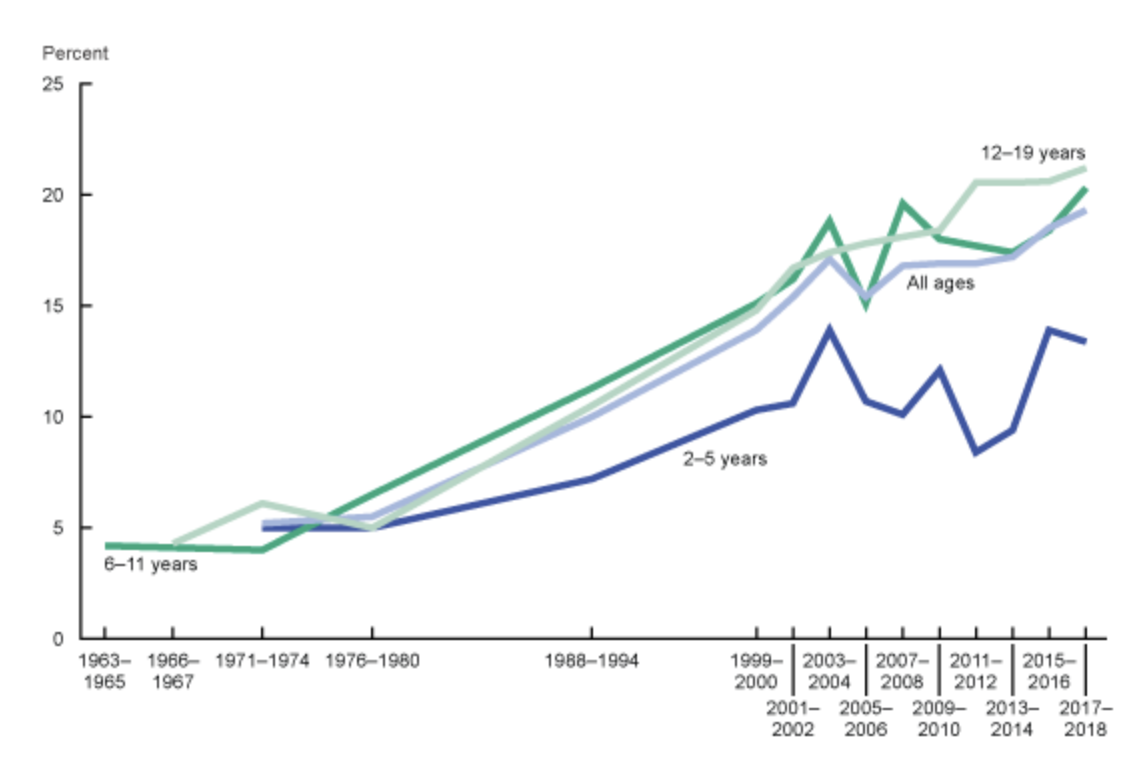
The obesity rate among U.S children aged 2-19 years old, 1963-1965 through 2017-2018. (Source: National Center for Health Statistics)
Childhood obesity is a serious public health issue because it affects the physical and mental health of children, and it can have major ramifications for their adulthood health. Obesity can lead to high blood pressure, diabetes, and other illnesses later in life. Childhood obesity could also cause mental problems such as depression and poor self-esteem. Simmonds et. al.’s study suggested that a person with a history of childhood obesity is five times more likely to develop obesity in adulthood than those without a history of childhood obesity.
Causes of Childhood Obesity
Children are more susceptible to external environmental influences because they are immature and not financially independent. The causes of childhood obesity can be categorized as lifestyle issues, family influences, and socioeconomic factors.
- Lifestyle issues: The leading causes of childhood obesity are the same as common obesity. Having unbalanced or unhealthy diets—for example, consuming high-calorie foods, candies, and sugar-sweetened beverages—cause excess weight gain. Physically inactive children are at risk of developing childhood obesity.
- Family influences: Highly controlled parental feeding styles—including pressuring or forcing children to eat and rewarding them with food—increase the prevalence of childhood obesity. The study also found that parents preferred to buy high-calorie, low-nutrient food for their kids because they believed their kids would like such kinds of food.
- Socioeconomic factors: The Centers for Disease Control and Prevention (CDC) states that a lack of access to public facilities increases the childhood obesity rate. About 40% of U.S households do not have full-service grocery stores within their communities. In this case, children are more likely to consume fast food and frozen food rather than fresh fruits and vegetables. More than half of U.S families do not have access to public infrastructures such as parks and playgrounds. Hence, children spend more time on sedentary activities (watching TV and playing video games), which negatively influences their health.
Healthy, Hunger-Free Kids Act of 2010 (HHFKA)
Healthy, Hunger-Free Kids Act of 2010 (HHFKA) promotes low-income children’s access to nutritious food by authorizing financing for federal school lunch and child nutrition programs. The US Department of Agriculture (USDA) reports from 2012-2013 show that 21.5 million U.S students received free or reduced-price meals at school under the influence of the HHFKA. The main terms of the Healthy, Hunger-Free Kids Act of 2010 are as follows:
- Implementing nutritional standards: The HHFKA enables the USDA to establish nutritional guidelines for any meals that are offered at schools, including products provided in vending machines and school stores. Schools receive funding to improve nutrient content in school lunch programs and the accessibility of drinking water.
- Expanding the beneficiary group: More than 115,000 students who satisfy income standards using Medicaid data are enrolled in the school lunch program. HHFKA increases meal plan access to students in low-income communities by simplifying eligibility criteria. At-risk students who are enrolled in after-school programs are also eligible for meal support.
- Increasing program professionalism: HHFKA requires a three-year cycle for school audits to monitor adherence to nutritional standards. Schools are required to provide transparent nutritional information on school meals to parents. HHFKA also provides school food service providers with instruction and technical support.
According to Kenney et al.’s study, HHFKA impacted many students in poverty. The prevalence of childhood obesity among impoverished students began to decrease after implementing HHFKA at 9 percent each year. The obesity rate among non-impoverished students was no different during the study period. The study revealed that with the regulation of HHFKA, overall childhood obesity is rising more slowly than expected.
Supplemental Nutrition Assistance Program (SNAP) and Other Childhood Obesity Federal Programs and Policies
Supplemental Nutrition Assistance Program (SNAP), the largest nutrition program in the country, offers short-term financial assistance to people who are struggling to pay for food. More than 43 million individuals received help from SNAP in getting access to food and drinks to maintain a healthy and balanced diet. Additional federal policies and programs that help children in the U.S get access to nutritious food and reduce the food insecurity rate and obesity rates among them are listed below.
- Child Nutrition Policies: Child nutrition policies vary from state to state, but their common goal is to reduce the food insecurity rate and provide children with nutritious food. Evidence shows that children’s food insecurity decreased by 33% half a year after their families received SNAP benefits.
- The Child and Adult Care Food Program (CACFP): Childcare facilities and other programs that provide nutritious food for children and adults receive federal funding from CACFP for compensation. In one day, over 4.2 million children have access to nutritious meals and snacks each day through CACFP.
- Dietary Guidelines: The first edition of the Dietary Guidelines for Americans (DGA) 2020-2025 provides nutritional recommendations for people at different life stages. The DGA recommends that children under two do not consume food and beverages with added sugar. The DGA also provides nutrition standards for federal nutrition programs and health policies.
- Women, Infants, and Children (WIC) Program: WIC provides the same benefits as SNAP to a different population. WIC promotes breastfeeding and provides healthy foods and nutrition education to eligible pregnant, postpartum, and breastfeeding women, infants, and children under five years old with healthcare and social services to help them maintain a healthy weight. The obesity rate for children ages 2 to 4 years that receive WIC benefits reduced by 1.5% from 2010 to 2018.
Challenges of SNAP
Under a new USDA policy, only people who benefited from the Temporary Assistance for Needy Families (TANF) program are able to receive SNAP benefits. Because of that, more than 3 million people lost SNAP eligibility. SNAP is funded through block grants, which means the level of funding is set across a designated time period. This could pose a challenge if the SNAP-eligible population grew quickly, like during a recession. Eligibility standards vary state to state, so two SNAP participants who live in different states may receive different benefits even if they have the same circumstances.
Benefits of SNAP
SNAP reduces poverty and food insecurity, and improves children’s health, indirectly reducing the childhood obesity rate. Children in SNAP-eligible households gain access to nutritious food and drink, which helps them develop healthy eating habits. Children who participated in SNAP also have a decreased risk of developing high blood pressure, heart diseases, diabetes, and other health diseases across their lifetime