This brief was originally published by Katrina Freeman on October 7, 2021. It was updated and republished by Pamela Pamela Nwakakwa on June 23, 2022.
Introduction
Across the world, approximately 38 million people are living with Human Immunodeficiency Virus (HIV). HIV is the virus which causes Acquired Immunodeficiency Syndrome (AIDS). It is spread through bodily fluids, which enter the bloodstream through a mucous membrane, open cuts or sores, or by direct injection. The most common ways to contract HIV are through:
- Participating in vaginal or anal sex with someone who has HIV without using a condom or taking medicines to prevent or treat HIV.
- Sharing injection drug equipment, such as needles, with someone who has HIV.
Newborns can contract HIV if their mother is HIV positive through breastfeeding, but this is preventable through early intervention.
“HIV can affect anyone regardless of sexual orientation, race, ethnicity, gender, age, or where they live. However, certain groups of people in the United States are more likely to get HIV than others because of particular factors, including the communities in which they live, what subpopulations they belong to, and their risk behaviors.”—HIV.gov
While HIV/AIDS was once considered a death sentence, medical advances such as ART (anti-retroviral treatment) and PrEP (pre-exposure prophylaxis) have allowed people with the virus to live long lives. Access to these medications are limited, and in some cases the stigma associated with HIV can prevent people from seeking more information or treatment, even if it is available.
US Response to Global HIV/AIDS
The United States funds HIV/AIDS prevention and treatment across the world. The US government donated billions of dollars to the Global Fund, funded PEPFAR programs, and worked alongside UNAIDS to stop the spread of HIV.
- The Global Fund is a multilateral partnership between governments, the private sector, and NGOS designed to end the AIDS, tuberculosis and malaria epidemics. The Fund allocates resources to local organizations combating these diseases. Since its founding in 2002, the United States has been the largest donor, contributing $17.6 billion. The United States has also shaped its policies as a member of the Global Fund’s Board. The Global Fund also works hand-in-hand with the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR).
- PEPFAR: President George W. Bush announced the creation of The U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) in 2003, and it was signed into law with bipartisan support. At the time, PEPFAR was the the “largest commitment by any nation to address a single disease in history” and has allocated “$85 billion in the global HIV/AIDS response, saving over 20 million lives, preventing millions of HIV infections, and achieving HIV/AIDS epidemic control in more than 50 countries around the world.” PEPFAR became the center for the American response to AIDS in Sub-Saharan Africa.
The Bush Administration hoped PEPFAR would be the medical version of the Marshall Plan, in terms of its scope and impact. “Localization” or shifting decision making powers and implementation away from the United States and towards local leaders and individuals, has been a goal for the organization. Local ownership is considered critical to meet global health and development goals, but there are implementation challenges which have hindered progress.
PEPFAR has been reauthorized through three different Administration’s and has become a cornerstone of American global health policy. The original program worked with 15 countries, and the program has expanded to include 60 countries in 2021.
- UNAIDS: 90-90-90 Initiative: the United States also worked alongside UNAIDS to implement their 90-90-90 initiative. This initiative includes a focus on viral suppression because viral suppression means that a person does not spread the virus. This is key to ending the epidemic. By 2020 this initiative set a goal where:
- 90% of all people living with HIV know their HIV status.
- 90% of all people with diagnosed HIV infection receive sustained antiretroviral therapy.
- 90% of all people receiving antiretroviral therapy have viral suppression.
As of the end of 2020, UNAIDS did not meet its goal. UNAIDS reports that in 2020, of all people with HIV worldwide:
- 84% knew their HIV status
- 73% were accessing ART
- 66% were virally suppressed
US Response to Domestic HIV/AIDS
In the United States, new HIV infections are highly concentrated among men who have sex with men; minorities, especially African Americans, Hispanics/Latinos, and American Indians and Alaska Natives; and those who live in the southern United States. Social determinants of health and stigma against the LGBT community and drug users can impede access to care. A key tenant to ending HIV is ensuring that patients know their status and have access to both ART and PrEP to ensure they do not spread HIV to their partners.
- Ending the HIV Epidemic in the US (EHE): this program is the coordinating body for the American government’s cross-agency response to domestic HIV transmission. It aims to “reduce the number of new HIV infections in the United States by 75% by 2025, and then by at least 90% by 2030.” The HHS Office of the Assistant Secretary for Health is coordinating this response as well as the following agencies, who are working together to reduce domestic HIV infections.
- Centers for Disease Control and Prevention (CDC)- CDC is working with local and state governments, federal partners, communities, people with HIV and people at risk of getting HIV in order to increase the use of EHE’s strategies
- Health Resources and Services Administration (HRSA)-HRSA’s Health Center Program and Ryan White HIV/AIDS program play an important role in carrying out EHE’s initiative through funding and providing HIV/AIDS services
- Indian Health Service (IHS)-IHS concentrates its EHE efforts on organizing and promoting HIV prevention and treatment activities in the communities that are most affected as part of an extensive public health approach
- National Institutes of Health (NIH)-NIH supports implementation science research done with community partners in EHE jurisdictions to decide what is the best way to use the very effective tools that are already available to deal with HIV
- Office of the HHS Assistant Secretary for Health (OASH)- OASH provides project management and coordination as a whole and keeps track of progress and delivers information through HIV.gov
- Substance Abuse and Mental Health Services Administration (SAMHSA)- SAMHSA is using its knowledge to address the intersection of substance use disorders and HIV in order to make sure that the right behavioral health interventions get implemented as part of EHE’s goal
The Ending the HIV Epidemic initiative focuses on four key strategies that, implemented together, can end the HIV epidemic in the U.S: Diagnose, Treat, Prevent, and Respond.
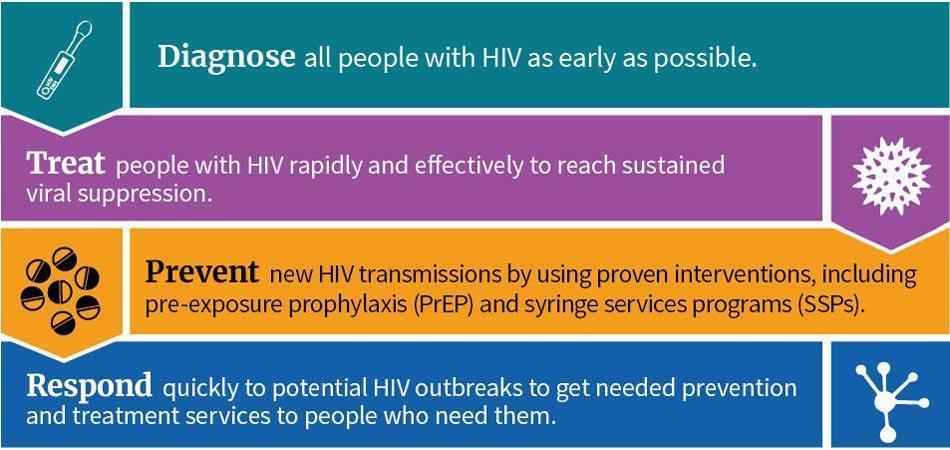
Source: HIV.gov
The CDC writes:
“Our nation faces an unprecedented opportunity once thought impossible. The most powerful HIV prevention and treatment tools in history are now available. Areas where HIV transmission is occurring most rapidly can also be identified. By deploying those tools swiftly and to the greatest effect, the HIV epidemic in America can end.”