No continent is experiencing as much difficulty with COVID-19 vaccination roll-out as Africa. As of September 14, 2021, there were 8.06 million COVID-19 cases recorded in Africa. In the week of September 12, there were 125,000 new cases. Though this was a 27% drop from previous weeks, weekly new cases are still as high as they were during the peak of the first wave. Currently, 19 African countries continue to report high or fast-rising numbers while the highly transmissible Delta variant has been found in 31 countries.
The continent as a whole is currently standing at a low COVID-19 vaccination rate, with only 3.6% of its population fully vaccinated. COVID-19 vaccines are provided to Africa via the COVID-19 Vaccines Global Access (COVAX) scheme. This scheme is a joint venture between the World Health Organization (WHO); Center for Epidemic Preparedness and Innovation (CEPI); Gavi, the Vaccine Alliance; and UNICEF. COVAX has a bulk purchasing program that is meant to allow smaller nations to get vaccines at the same price as larger countries. 92 of the world’s poorest nations depend on COVAX to secure vaccines.
Worldwide Vaccine Shortage
COVAX’s main promise was that by the end of 2021, 20 percent of the world’s population would be vaccinated—620 million doses. Wealthy nations fund COVAX in return for secured vaccine shipments in the future. Many had signed deals with manufacturers as early as July 2020, while COVID-19 vaccines were still in development and undergoing trials. Buying up large quantities of the vaccine far in advance has dried up the supply, leaving nothing for poorer nations. Due to this lack of supply, COVAX has only been able to distribute 65 million vaccines to over 100 countries. The primary supplier of vaccines to COVAX, the Serum Institute of India, has exported more vaccines than it has given to the entire Indian population, and due to this discrepancy, they have halted delivering vaccine shipments to other countries.
Larger countries with poorer populations are falling behind in vaccine distribution compared to more wealthy nations with smaller populations. It’s estimated that poorer countries will not get broad access to vaccines until 2023 or 2024.
Africa has received just 276 million doses and administered 198 million. Currently, less than 10 percent of African nations are expected to meet the end-year goal of fully vaccinating 40 percent of their population.
WHO Regional Director for Africa, Matshidiso Moeti, warned about the consequences of not getting vaccines to places like Africa, saying “the staggering inequity and severe lag in shipments of vaccines threatens to turn areas in Africa with low vaccination rates into breeding grounds for vaccine-resistant variants. This could end up sending the whole world back to square one.” However, world leaders at the Global COVID-19 Summit in September announced that they would pledge hundreds of millions of doses to low- and lower-middle-income countries through COVAX in the next year.
Unusable Vaccines in Africa
Even when some vaccines are able to make their way to Africa, problems arise. Many African countries have had to either destroy or return thousands of vaccine doses because they had exceeded the expiration date. For example, Malawi destroyed 20,000 doses of the AstraZeneca vaccine and South Sudan announced that it would destroy 59,000 doses. These countries had both received vaccines from the African Union, which receives vaccines from other nations as well as manufacturers. Many of the vaccines donated through COVAX had already gone bad. The Democratic Republic of Congo said that it could not use most of the 1.7 million vaccines it received under the COVAX scheme for poorer countries. Also through COVAX, South Sudan received 132,000 doses of the AstraZeneca vaccine in March with an expiration date at the end of June. South Sudan did not have the ability to undergo a mass vaccination rollout in such a short period of time, so it handed back 72,000 of those doses.
In South Africa, one million doses were received from India in February, with an expiration date of April. The government, however, was concerned that those vaccines would not protect against the South African COVID variant, and so, in late March, the doses were passed on to other African countries such as South Sudan, Nigeria, Togo, Ghana, and The Gambia. Although Togo and The Gambia were able to use all of their vaccines prior to the expiration date, larger nations were unable to use all theirs.
Vaccine Mobilization and Skepticism
Other than receiving almost-expired vaccines, many African countries were unprepared to undergo such a vast vaccine mobilization program. These nations know how to vaccinate, but many do not have sufficient financial resources and are plagued by an ineffective government, poor transportation networks, and poor health services. There has been trouble with training health care workers and convincing them to take the vaccine. Concerns over the safety and efficacy of vaccines, fueled by myths and false information, have long plagued many nations in Africa, particularly Sub-Saharan ones. These myths have created distrust among communities and generated a dangerous environment for increased COVID transmission rates.
The Africa CDC conducted a study on COVID-19 vaccine perceptions in 15 countries that indicated a significant proportion of those living on the African continent express concerns over vaccine safety. Respondents tended to view new COVID-19 vaccines as less safe than vaccinations in general. For example, while 94 percent of Ethiopian respondents said they would be willing to take the COVID-19 vaccine, other nations rated lower. The Democratic Republic of the Congo had only a 59 percent willingness to get vaccinated. More than half of respondents surveyed felt that the threat from coronavirus is exaggerated and that it does not pose the risk that others claim. Moreover, 41 percent of respondents mentioned online sources as their most trusted source for information about COVID-19, and respondents who demonstrated vaccine hesitancy were more inclined to consult online sources than those who were willing to take the vaccine. The problem seems to be a lack of education about the effects and transmissibility of the virus.
Impacts on International Development
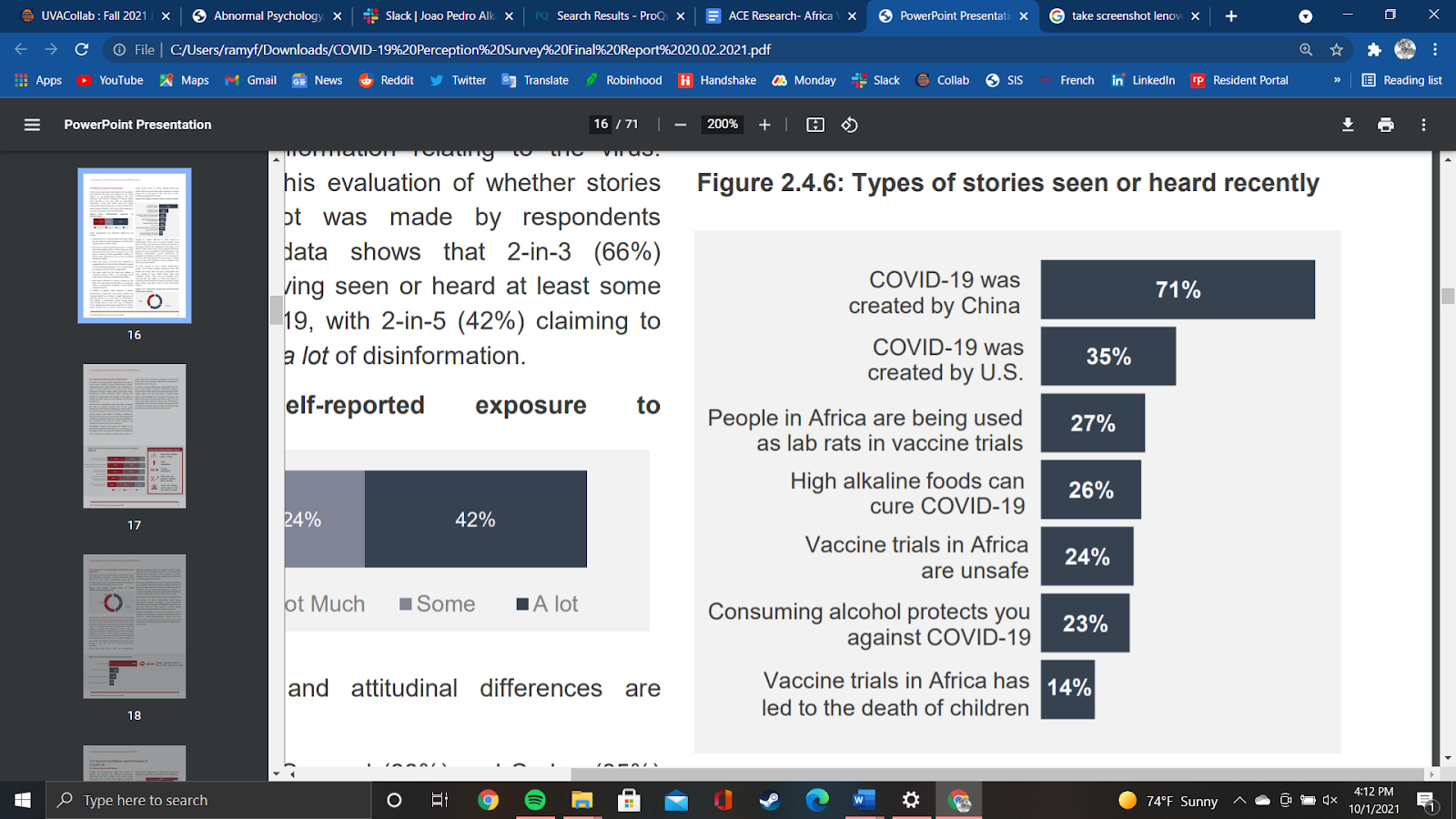
There could be a greater force affecting people’s perceptions about the virus. In the same study by the Africa CDC, a survey was conducted to find out the exposure to general misinformation regarding COVID in Africa. Unsurprisingly, the most popular story heard on this continent, and other continents too, was that COVID-19 was created by China. The second most popular was that the virus was created by the United States, and the third was that people in Africa are being used as lab rats in vaccine trials.
These rumors reveal something deeper about how people in Africa perceive the West. Throughout history, Africa has been exploited by Western nations through the global slave trade and the Scramble for Africa, which saw European powers divide the continent for their own commercial and political interests. These two major historical events had direct consequences on the development of Africa, and the continent has not forgotten the injustices it had to endure. Anti-Western sentiment stems from centuries of colonization, occupation, and intervention. The reluctance to trust Western countries in providing vaccines for a novel virus is unsurprising given these facts.
A healthy diet requires an appropriate balance of macronutrients, micronutrients, and caloric intake. A proper diet can reduce the prevalence of nutrition-related diseases such as diabetes, obesity, hypertension, and heart disease. In the United States, people in the carceral system experience a disproportionate amount of diet related illnesses. A special report by the United States Department of Justice found that 30% of incarcerated people have hypertension compared to 18% of the general population, 9% have diabetes compared to 6.5% of the general population, and 9.8% have heart problems compared to 2.9% of the general population. One factor suspected of contributing to this increased incidence of diet related illness is the high availability of processed foods and the limited availability of fresh fruits and vegetables in their prison diet. Processed foods are more frequently served in prisons due to cheap costs and long shelf life. Most correctional facilities and prisons outsource to private food vendors. Prison meals outsourced in this way are mass produced and cost around $1-$2 per meal.
Background Information
While processed foods are cheaper and more easily sourced, they tend to have high levels of sugar, cholesterol, and sodium, and limited amounts of essential micronutrients such as potassium, magnesium, and vitamin E.
In 2016, the California’s Department of Corrections food administrator stated the sodium content of meals averaged 3,500 milligrams per day. For reference, the United States Department of Agriculture (USDA) advises people to eat up to 2,300 milligrams per day.
A 2012 analysis of South Carolina correctional facilities found that inmates received an average of 97.5 grams of sugar per day, more than double the USDA’s recommended 41.8 grams.
While fruits and vegetables provide many micronutrients, prisons are often reluctant to purchase them because of their short shelf-life and limited seasonal availability. According to a report conducted by Impact Justice, around 62% of incarcerated individuals stated they rarely have access to any fresh vegetables, while 54% expressed that they rarely had access to fresh fruits.
One way that prisons in the U.S. can offer healthier foods to incarcerated people is through prison agricultural programs. These are programs that connect prisoners with local farms. Through prison agricultural programs, incarcerated people can gain agricultural skills, provide fresh food to the prison population, and give back to the community by providing support to local farms.
One such program is Planting Justice, which works to build gardens and create jobs for people transitioning from prisons in San Francisco. Individuals who go through the program have a 0% recidivism rate compared to the general 44.6% recidivism rate in California. Planting Justice provides a living wage to current and formerly incarcerated participants entering the program. Another prison agricultural program is Salvation Farms, an organization that partners with the Vermont Department of Corrections. Salvation Farms provides education, an outlet for productivity, and agricultural goods to incarcerated people. It aims to bridge the gap between agricultural surpluses and food distribution systems by partnering with various organizations and institutions across the food sector. By partnering with the Vermont DOC, Salvation Farms is able to provide fresh produce to incarcerated people in Vermont.
Positive Arguments of the Programs
These programs improve nutritional quality for incarcerated people who choose to consume more fresh fruits and vegetables. This could potentially reduce the percentage of incarcerated people with diet related diseases and the healthcare expenditures associated with those diseases.
Prison agricultural programs can teach incarcerated people employable skills. Having those skills may lead to a reduction in recidivism if formerly incarcerated people have access to stable employment when re-entering society. The education received may also translate to healthier eating habits after re-entry into communities.
Prison agricultural programs also provide an outlet for productivity, which can potentially improve the mental health of incarcerated people participating in agricultural related activities.
Negative Arguments
On the other hand, there’s debate over whether or not the net costs of prison operations are reduced when implementing prison agricultural programs. According to the correctional spokesperson for Wyoming County Correctional Facility, the farm that worked with the correctional facility lost $3.4 billion per year. In addition, security costs play a factor; extra security is needed when incarcerated people are working on the farms. Additionally, while fruits and vegetables are integral to nutrition, proteins and grains are also essential to a nutritious diet. Therefore, prison agricultural programs may fix some, but not all of the nutritional deficiencies present among incarcerated populations.
Pay for performance (P4P) is a healthcare payment model that offers financial incentives to healthcare providers that meet certain performance measures. A wide range of healthcare providers are eligible to participate in P4P programs, including physicians, hospitals, and medical groups. Performance measures are predetermined evidence-based practices that lead to better patient health outcomes. Successfully meeting these performance measures should, in theory, lead to better patient health outcomes. The main objective of P4P programs are to lower healthcare expenditures while simultaneously improving patient health outcomes. There are two basic types of P4P programs: the first type provides financial incentives to healthcare providers if they meet performance measures, while the second type financially penalizes healthcare providers for bad practices and bad outcomes. Consistent positive associations between P4P programs and patient health outcomes have not yet been achieved in any healthcare setting. While some studies have shown that P4P programs produce positive results in ambulatory settings, results are often inconsistent across studies, the magnitude of the effect is not significant, or methodological flaws make results difficult to interpret. At the moment, there is currently no clear evidence that patient health outcomes will improve through implementing P4P programs.
Fee For Service Vs. Pay for Performance:
No country spends more on healthcare than the United States. In 2018, healthcare expenditures totaled 3.6 trillion dollars, averaging $11,172.00 per person, and accounting for 17.7% of Gross Domestic Product (GDP). Despite this, Americans experience poor health outcomes, compared to citizens from other high income countries (as defined by the World Bank). Relative to 10 other high-income countries, the US has the highest number of hospitalizations from preventable causes like diabetes and hypertension, the highest rate of avoidable deaths, the highest chronic disease burden, the highest obesity rate, and the lowest life expectancy. One solution proposed by United States policy makers to address high healthcare expenditures and negative patient outcomes is to implement large scale P4P programs.
P4P programs emerged in the early 2000s as an alternative kind of healthcare reform, deviating substantially from the traditional fee for service (FFS) healthcare payment models. P4P programs focus on issuing bonuses and penalties to healthcare providers, based on their adherence to performance measures and their patient health outcomes. This differs from FFS approaches, which pay healthcare providers universal rates regardless of patient health outcomes or financial efficiency. FFS systems are criticized for promoting healthcare providers to administer as many services as possible. This can lead to unnecessary spending on medical equipment, personnel, and facilities; substantially driving up healthcare costs while offering a marginal improvement of patient health outcomes.
For example, the United States has the second-highest number of MRI units per capita, at 40 MRI units per million people. This is more than four times the number of MRI units per capita in Canada. Similarly, Canada also has three times less cardiac surgeons per capita than the United States. This is due to the Canadian government restricting the number of MRI machines that hospitals can buy, and limiting how many hospitals can have open-heart surgery facilities. This forces Canadian healthcare providers to ration these services to patients that need them the most. Despite having three times more cardiac surgeons and performing far more cardiac surgeries than Canada, the survival rate of patients with myocardial infarctions (heart attacks) in the United States marginally differs. Critics argue that cases such as the one above demonstrate that FFS systems lead to healthcare overspending.
Performance Measures:
To counteract healthcare overspending, proponents of P4P programs advocate the use of performance measures in order to determine the amount of funding that healthcare providers receive. The most common type of P4P program rewards healthcare providers for meeting predetermined performance measures, usually in the form of bonuses and increases in funding. Performance measures tracked by P4P programs can be divided into four subcategories: process measures, outcome measures, patient experience measures, and structural measures.
Process measures refer to clinicians’ performance of evidence-based practices that lead to positive patient health outcomes. An example of a process measure could be examining whether or not patients were counseled to quit smoking during an annual physical, determining how often healthcare providers check the blood pressure of patients that are admitted to the emergency room, and analyzing how accessible early detection cancer screenings are to at-risk patients.
Outcome measures analyze certain end results following the administration of aftercare.An example of an outcome measure could include heart attack survival rates among patients admitted to the emergency room.
Patient experience measures refer to patients’ perceptions of and satisfaction with the quality of care they receive.This can include patients’ perception of the quality of communication with their providers and the cleanliness and quietness of their rooms.
Structure measures consider the physical facilities and equipment used during the care delivery process, an example being whether or not providers use health information technology.
Alternatively to issuing bonuses, pay for performance programs may also penalize healthcare providers for negative performance measures. Such penalties can include a reduction in funding and a reduction in services that the healthcare provider in question can offer. Negative performance measures can include poor patient health outcomes, medical errors, and inefficient spending.
Potential Benefits and Consequences of Implementing Pay for Performance Programs:
There are many debates both for and against implementing P4P programs. Proponents of P4P programs maintain that it is necessary to move away from FFS programs in order to eliminate the possibility of providers taking advantage of pay-by-volume approaches for healthcare funding. Such funding systems can lead to gross overspending, driving healthcare expenses up and ultimately making healthcare less accessible due to high costs.Furthermore, FFS programs often neglect preventative care’s role in improving patient health outcomes and minimizing healthcare expenditures. Many of the performance measures outlined in the section above embrace preventative care principles, which further incentivizes healthcare providers to focus on preventing diseases rather than treating them. P4P programs can be specifically designed to increase healthcare transparency through publicly reported metrics.This is beneficial for patients because it encourages provider accountability and motivates providers to strengthen their reputations, while building competition through consumer-informed choice.
In some areas, P4P has proved effective at decreasing negative patient outcomes. For example, 30-day hospital readmission rates have been falling since 2012 following the implementation of large scale P4P programs. However, while P4P programs have advantages, there are also criticisms against such programs. One of the most notable objections towards implementing P4P programs is that quality of care may be sacrificed for the sake of meeting performance measures. Critics have expressed concerns about the exacerbation of disparities as providers become disincentivized to treat certain populations that may not perform well on P4P measures. Similarly, more severe or complicated patients may be avoided, or patients who need end-of-life care may not receive it until the measured time period is complete, so as not to impair providers’ statistics. Another concern is the difficulty of measuring quality of care. There is controversy surrounding how effective performance measures are, since patient health outcomes can be affected by many external factors that are beyond healthcare providers’ control. Additionally, some P4P programs analyze financial performance measures separate from patient related performance measures. Certain performance measures may appear paradoxically good, despite a negative patient outcome. For example, financial performance measures may classify a patient that dies soon after an operation as more cost-efficient than a patient who is healthy but needs longer postoperative care prior to being discharged.
It’s inconclusive how effective P4P programs are at improving patient outcomes. A P4P demonstration project by the Centers for Medicare and Medicaid Services in partnership with Premier Inc. compared 260 hospitals that had implemented P4P programs against a control group of 780 hospitals that operated traditional FFS programs. The performance of hospitals implementing P4P initially improved more than the control hospitals, with more than half of P4P hospitals reaching high-performance scores while less than a third of control hospitals achieved high scores. However, by the fifth year of the program there was virtually no difference between the performance scores of P4P hospitals and control hospitals. Though P4P shows a lot of potential, evidence for its benefits is not conclusive, and more research is warranted regarding the outcomes of P4P programs, from both short-term and long-term perspectives.
Value-based care is an overarching term for any healthcare delivery model in which payment is based on health outcomes, as opposed to the volume of services provided. The American healthcare system largely operates on a Fee-for-Service system. In this system, providers are paid based on the services they offer. Although this allows for a simpler billing process, and easier communication between providers and insurance organizations, it also has potentially problematic implications regarding the priorities of healthcare providers. Fee-for-Service reimbursement incentivizes billing for a large quantity of services, without taking into consideration the quality of the care or its associated health outcomes. The goal of value-based care is to reconcile the incentives provided by healthcare reimbursements with the overarching goals of healthcare promotion and disease prevention. As such, value-based care models often incentivize proven high-quality measures such as the use of preventive services, coordination of care, and an emphasis on patient satisfaction, with incentives linked to health outcomes rather than services rendered.
The Affordable Care Act, which was passed in 2010, opened the door for many mechanisms that promoted value-based care, and gave both payers and providers the necessary infrastructure to implement it. Some important mechanisms include the Medicare Access and CHIP Reauthorization Act (MACRA), Bundled Payments, and Accountable Care Organizations.
MACRA
The Medicare Access and CHIP Reauthorization Act (MACRA), which was passed in January 2015, laid the groundwork for much of the value-based care infrastructure that we see today. MACRA established quality payment programs, which incentivize payers and providers to implement value-based reimbursement models. There are two types of quality payment programs:
An alternative payment model (APMs) is any payment approach that creates incentive for clinicians to deliver high-quality and value care. Advanced APMs are specific types of APMs where this incentive is created by allowing providers to take on more risk. This means that providers take on greater responsibility for their patients’ health outcomes, but they also get the opportunity to share in savings associated with maintaining patient health. In doing so, patient care becomes centered around maintaining patient health rather than just rendering potentially unnecessary services.
Merit-based incentive payment system (MIPS) dictates how physicians receive reimbursements when treating Medicare patients. Incentives and penalties are built around a weighted average of performance measures, such as quality of care, clinical practice improvement practices, cost of delivery and resource use, and interoperability and meaningful use of electronic health records.
Bundled Payment
Bundled payments are an alternative payment model in which the total price for an episode of care is predetermined. An episode of care is the entire continuum of care associated with a specific condition’s treatment. For example, all of the services associated with a joint replacement, from the initial consultation to rehabilitation, would fall under one episode of care. In this model, providers assume additional risk, meaning that they incur a loss if patient care costs more than the initial price point, and make a profit if it costs less. The incentives of bundled payments are completely different from that of fee-for-service care, since providers must implement high-value clinical interventions to save money, rather than simply increase the volume of services they offer.
Bundled payment models first became prominent after the implementation of the Center for Medicare and Medicaid Services’ (CMS) Bundled Payment for Care Initiative (BCPI); this came after the passage of the ACA. This program offered bundled payments for Medicare patients that underwent Acute, Post-Acute, and Prospective Acute care episodes. These initiatives proved effective in reducing the cost of care and incentivizing high value practices, such as preventive care and coordination of care. For example, the cost of joint replacement episodes decreased by 20.8% under the BCPI post-acute care bundle. Seeing the early success of BCPI, CMS and private payers are beginning to implement more bundled payment models, with 17% of healthcare payments having been done under bundled payment in 2021.
Accountable Care Organizations
Accountable care organizations are networks of physicians, clinicians, and larger healthcare systems, in which all parties share responsibility for quality, cost, and coordination of care. Providers in this system must coordinate with government agencies and community-based organizations to promote population health in their catchment area. ACOs operate in a shared savings model. This means that spending on specific patients is assigned a total cost of care (TCoC) benchmark based on factors like their pre-existing health conditions and historical spending; members of the ACO share in any savings when the cost of successful care falls under the TCoC. In order for members of the ACO to share in the savings, they need to meet 30 quality measures. As a result, ACOs help ensure the administration of high quality care, while also incentivizing preventive care through their shared savings model.
E-cigarettes, or nicotine vapes, are electronic devices used to deliver nicotine to the user’s lungs, where it can be readily absorbed. Nicotine is the addictive chemical found in tobacco products. At its most basic, an e-cigarette is composed of a mouthpiece, a cartridge, a heating element, and a battery. The cartridge holds the e-liquid, in other words a mixture of nicotine, water, vegetable glycerin or propylene glycol (or both), and flavorings. When activated, the heating element draws on the battery’s power to turn the liquid into vapor, where it is then pulled into the user’s lungs via the mouthpiece.
Proliferation in the US
The first mention of an e-cigarette occurs in a patent from 1930, which was never commercialized. In 1998, a major US tobacco company requested Food and Drug Administration approval to bring their version of the e-cigarette to the market, which the FDA denied on the basis of it being an unapproved drug delivery system. This resulted in a lull in the market for nicotine vaporizers, but momentum resumed in 2003 in Beijing, China, with the first commercially successful rendition of the e-cigarette. E-cigarettes were introduced to Europe and the United States in 2006. In the years since 2006 there has been a flurry of commercial success for e-cigarettes, and they are now a popular consumer product in the US, with ongoing research as to their health effects and how they are best regulated.
Impact on Health
Because e-cigarettes only gained commercial success in the early 2000s, there is limited long-term data on the health effects of vaping nicotine. That means there are no certain long-term conclusions about health that can be drawn. However, assumptions can be extrapolated from available long-term data on similar types of exposure, such as exposure to artificial fog machines or food vapors in a factory setting.
Flavoring agents: One such example is a condition commonly called “popcorn lung”, a form of life-threatening respiratory failure so named because it was first observed in popcorn factory workers who had inhaled a flavoring agent called diacetyl. Diacetyl was found in the majority of sweet e-liquids evaluated by one study. Many ingredients in e-liquids, like diacetyl, are rated by the FDA as “generally recognized as safe” (GRAS) when eaten but are untested for inhalation in an aerosolized form. This is true of vegetable glycerin and propylene glycol as well, and these knowledge gaps are common when it comes to e-cigarettes.
Product labeling issues: There are also numerous inconsistencies in product labeling, making it even more difficult to know exactly what one is inhaling. Nicotine concentrations in e-liquid, for one, have frequently been found to differ from the labeling. E-liquid typically contains 16-24 mg/ml of nicotine, although the available concentrations range from 12-100 mg/ml. The average cigarette, on the other hand, delivers approximately 2 mg of nicotine to the smoker, and the median fatal dosage for an adult is around 60 mg. High concentrations of nicotine in e-liquid have caused an increasing frequency of nicotine poisoning from accidental ingestion of e-liquids among children and adults.
Metal leakage: The frequent heating and cooling process of the e-cigarette heating element can cause metals such as chromium, manganese, nickel, and lead to gradually leech into the e-liquid as the heating coil breaks down. Inhalation of these metallic fumes by welders is known to increase respiratory illness and possibly increase the incidence of lung cancer. A similar phenomenon could be extrapolated to e-cigarette users, although more research is required.
Other ingredients: Overall, e-cigarettes contain lower levels of carcinogens than conventional cigarettes, but comparable levels of ultrafine particles and other toxins that affect cardiovascular health and account for half of smoking related illnesses.
Enforcement of E-Cigarettes
From a public health standpoint, e-cigarettes present a challenge in that it is difficult to regulate indoor vaping or create “smoke free” areas, since e-vapor disappears quickly and the scents are not unique to e-cigarettes. A recent study found that 60% of e-cigarette users vape in “no smoking” areas, and e-cigarette vapor has been found to lower indoor air quality and result in similar levels of nicotine absorption in bystanders as second-hand cigarette smoke does. In recent years, there has been an increase in regulation surrounding vaping in public places, but enforcement is not easy.
E-Cigarettes as a Cigarette Substitution
E-cigarettes have the potential to be used as a smoking cessation aid, since research thus far shows them to be less dangerous than a traditional combustible cigarette, and the customizable dosage of nicotine they deliver can help ease a smoker’s transition off of traditional cigarettes. However, several meta-analyses show that they are only helpful in a specific context. E-cigarettes purchased over-the-counter as a consumer product by current smokers, both those who were motivated to quit smoking and those who were not, are not associated with increased smoking cessation among adults. However, when they are provided to smokers motivated to quit as a free therapeutic tool, they do result in a higher success of smoking cessation. Another meta-analysis found that there were a few studies that showed the opposite effect, although the authors stated that these studies did not account for the frequency of use. Higher frequency vaping is associated with more successful cigarette cessation. All studies concerning this topic emphasized that e-cigarettes are safer than combustible cigarettes, but not risk free either. It was unusual for people who had quit smoking with the help of a nicotine vape to then go on to quit vaping as well, with 80% of quitters continuing to vape. These studies suggest that regulatory authorities should make e-cigarettes available as a prescription therapy for current cigarette smokers, rather than a widely available over-the-counter recreational product. However, the unknowns when it comes to the long-term effects of vaping make employing the technology in a therapeutic context risky.
Despite therapeutic potential for smokers attempting to quit combustible cigarettes, there is some evidence that e-cigarettes have the effect of introducing non-smokers to nicotine, which is counterproductive from a public health standpoint. Youth e-cigarette use doubled or tripled every year between 2011-2014, and by 2014 e-cigarette use in youths had surpassed traditional cigarette use. Twenty-five percent of youths using e-cigarettes did not match the risk profile of youth cigarette smokers, suggesting that they would not have been introduced to nicotine if it had not been for the novelty, flavor variety, and perceived harmlessness of vaping, all of which are cited as unique reasons that youths are attracted to vaping.
Public Health Debates
Despite the e-cigarette being a relatively new commercial product, there is public contention regarding whether the therapeutic benefits of e-cigarettes outweigh the public health risks. There are generally two camps when it comes to assessing the risks and rewards of e-cigarettes: The first is concerned with easing the health burden on people already addicted to traditional combustible cigarettes, the other is concerned with preventing nicotine addiction in the non-smoking population. According to available data, traditional cigarettes are almost unanimously viewed as more harmful to the user than e-cigarettes. For this reason, if therapeutic nicotine vapes are a successful aid for traditional cigarette cessation, then their availability would help decrease the negative health burdens of combustible cigarettes. On the flip side, widely available nicotine vapes can also expose non-users to nicotine for the first time. So, in analyzing how e-cigarettes should be regulated, public health officials must determine how different forms of regulation impact the health of these two separate risk groups.
Regulating E-Cigarettes
The primary law regulating e-cigarettes in the United States is the federal Tobacco 21 law (T21). It was signed into place in 2019 by former president Donald Trump, and prohibits the sale of tobacco products, including e-cigarettes, to anyone under the age of 21 years. Although some state codes still list 18 years as the legal age to purchase tobacco products, federal law prevails in this case. T21 is a blanket regulation for the entire country, but individual states can tax e-cigarettes and other products deemed harmful to the general public. This type of tax is often referred to as a “sin tax,” and these taxes fall under the authority of state governments. Some items that are typically taxed to correct for their societal harm include tobacco, alcohol, and gambling. By raising the prices on these items through taxation, state governments can deter people from purchasing them even if they are legally allowed to do so. Further, the money generated by this “sin tax” can hypothetically go towards undoing some of the damage these products do to society, such as helping to pay for state tobacco control programs. In February 2020, the FDA issued a ban on the sale of cartridge-based e-cigarettes in flavors other than tobacco and menthol, since the more novel flavors, like fruit- and dessert-based flavors, were shown to be one of the features that spurred youths to take up vaping. Some states have further regulations surrounding where it is acceptable to vape, such as rules prohibiting vaping in “smoke free” areas, or within 500 feet of a premises primarily occupied by youths.
In 2006 when e-cigarettes were first making their commercial debut, they entered the market unregulated. As lawmakers were beginning to catch on to the risks of unregulated e-cigarettes, massive cigarette companies also entered the market, and their influence hindered legislative efforts. The initial opposition to state and local level regulation came from e-cigarette users and independent retailers, but the interference of large tobacco companies shifted the dynamics towards those of the tobacco control debates spanning the 1970s-1990s. These debates often cited “imminent” federal regulation which would render state policy obsolete, and used lobbying and campaign contributions to influence state-level regulation surrounding e-cigarettes. Another way that the government influences e-cigarette consumption is through projects like the FDA’s “The Real Cost” campaign, which uses scare-tactic advertising to mold the newer generation’s perception of smoking, targeting those aged 12-17 years. In 2017 the FDA pivoted from anti-cigarette messaging to launching a $60 million anti-vaping campaign, which follows the data revealing that e-cigarettes have been the primary form of nicotine consumption for youths since 2014. This campaign is some of the only federal intervention that targets the consumption side of e-cigarettes rather than the retail side, and has been compared to the 1936 anti-cannabis propaganda film “Reefer Madness”. This tactic may reduce vaping in youths, but it has the dual effect of spreading the inaccurate perception that e-cigs are equally or more harmful than traditional cigarettes, which can discourage adult smokers from using vaping as a quitting aid.
Health literacy is an individual’s ability to find, understand, and use information and services in order to make well-informed health-related decisions for themselves or others. Only about 12% of Americans are considered health literate. When health organizations provide patients health information that is difficult for the patient to understand, or has unfamiliar and confusing steps, we create a health literacy problem. Low health literacy is common among Americans who have limited education, are older, have lower socio-economic statuses, are non-native English speakers, and those with chronic medical conditions. Misinformation, which is false or inaccurate information that can deceive or misinform others, can create confusion, fear, and anxiety among those with low health literacy. It can even impact those who have high health literacy and their ability to understand medical information. Misinformation has arguably spread just as fast, or faster, than COVID-19 itself.
Health Literacy’s Importance During a Pandemic
Having a high rate of health literacy can help prevent the onset of illness and disease, reduce national disease averages, and improve population health. A current and persistent threat to global health is the COVID-19 virus, which has caused mass casualties and long-lasting negative health outcomes to the affected global population. There are currently 11 variants of COVID-19, with the Delta variant being of particular interest. Due to an increase in strains and total cases, a rapid transmission of accurate and reliable health information is crucial in preventing the virus from spreading further. Patients who don’t have access to accurate and reliable health information have higher hospitalization rates and develop more chronic diseases, on average. Similarly, Pfizer states that low health literacy is associated with many adverse health outcomes, such as:
Lower reported health status
Greater mortality rates
Less-specific disease knowledge and ability to recognize common signs and symptoms of illness.
Greater utilization of hospital services, and less confidence and skills needed for self-care and chronic disease management.
The Lancet notes that health literacy also involves taking social responsibility, as thinking beyond personal choices and self-interest can make an impact on reducing the rapid transmission of COVID-19 and increase vaccination rates. Health literacy provides the tools needed to prevent and combat these negative health outcomes, and allows patients to make educated decisions about their health.
Impact on Vaccine Development
The current goal is to get 75% of the world population vaccinated with one of the approved vaccines available; Pfizer-BioNTech, Moderna, and Johnson and Johnson/Janssen. Achieving this goal of 75% would mean that herd immunity could take effect, where enough people are protected from COVID-19 to effectively control its spread, thus reducing associated transmission and mortality rates. Currently, about 46.8% of the world has received at least one dose of the three vaccines listed. As of late September of 2021, Africa had the lowest vaccination rate, and Europe had the highest, with North America following closely behind. 79% of shots administered are in high or upper-middle-income countries, and 0.5% of doses were administered in low income countries. Low health literacy and misinformation have targeted individuals through social media, news outlets, word of mouth, etc. Some common misconceptions include:
The COVID-19 vaccine contains a microchip.
The vaccine can make an individual magnetic.
The vaccine can make an individual ‘shed’ vaccine components outside of the body.
The vaccine alters a human body’s DNA.
The vaccine alters a woman’s fertility.
The CDC notes that most of the misinformation and disinformation has been centered around vaccine development, safety and effectiveness, and COVID-19 denialism. In addition, the WHO calls the spread of misleading COVID-19 and vaccine information an infodemic, that furthers, “skepticism and distrust, which is the perfect environment for fear, anxiety, finger-pointing, stigma, violent aggression and dismissal of proven public health measures – which can lead to loss of life.” This scepticism and distrust has cost the United States over $5 billion from June-August of 2021 from preventable COVID-19 hospitalizations, and caused over 280,000 preventable cases among the unvaccinated during the same time period. Since the onset of the virus, nearly 4.8 million have lost their lives worldwide.
How to Monitor Misinformation
In order to make well-informed decisions about one’s health, access to reliable and factual health information is essential. Monitoring misinformation and disinformation during a global pandemic can be challenging, but there are strategies available to assist with this goal. The International Federation of Library Associations and Institutions (IFLA) recommends these 8 strategies to help spot misinformation:
Consider the source: identify the author (if possible) and investigate other publications the author has made. Is the author relevant and trustworthy?
Read beyond the story or publication, or compare other articles to it in order to increase validity.
Make sure the supporting sources are credible, and support the publication.
Identify if others agree: is it peer-reviewed, or trustworthy among others?
Try to identify if it is a joke/satire.
Check your biases, and consider your own beliefs as they could affect judgement.
Ask the experts: consult credible, trustworthy sources like the WHO, CDC, etc.
Read the article or story before you click share.
If one comes across a source that is spreading false information, there are ways to report it here, which provides instructions to report misinformation/disinformation among various social media outlets, like Facebook, Instagram, Twitter, YouTube, TikTok, etc.
Vaccination mandates are state laws that require children to be immunized against certain diseases prior to attending childcare facilities and public educational institutions such as daycares, preschools, elementary schools, middle schools, and high schools. Vaccines are prophylactic biological preparations that train the immune system to recognize and destroy certain pathogens. They often contain attenuated versions of the pathogen, toxins that are produced from the pathogen, or surface proteins that are naturally present on the pathogen. When an individual successfully vaccinates against a disease, they become protected from that disease for an extended period of time. Should a person come into contact with a disease that they are vaccinated against, they’ll experience either no illness or a weaker version of the illness.
Vaccines protect not only those who are vaccinated, but also those who are in close proximity to them. If a high percentage of individuals are vaccinated in a community, herd immunity can protect those who are not able to vaccinate due to abnormal medical conditions. Diseases that children are required to vaccinate against are often highly contagious, and may have high morbidity and mortality rates. Widespread vaccination is one of the best strategies for preventing large scale outbreaks of preventable diseases, and this is achieved through the implementation of vaccination mandates. Every state has the authority to mandate vaccines through police powers, and each state requires a specific regimen of vaccines that it determines necessary to protect the health of the public. States can also choose whether or not to offer medical, religious, and philosophical exemptions to these vaccination mandates, and dictate what steps parents must go through to acquire exemptions. States that offer easily accessible exemptions tend to have greater rates of preventable diseases.
Since the late 1980’s, vaccination mandates have prevented hundreds of thousands of deaths, millions of hospitalizations, hundreds of millions of illnesses, and trillions of dollars in direct/social costs related to illnesses and hospitalizations. Given the extremely high cost/benefit value, the federal government purchases vaccine doses for preventable diseases and provides them to uninsured/underinsured children free of charge through the Vaccines for Children Program (VFC). However, vaccines are neither perfectly effective nor completely safe. Some people who are vaccinated will still contract the diseases they are protected against, and some people will experience serious injuries or even death from standard vaccinations. Since society mandates that children be vaccinated before entering daycares and public educational institutions, federal lawmakers established the National Vaccine Injury Compensation Program (VICP) through the National Childhood Vaccine Injury Act (NCVIA) to compensate families of children who were injured by mandated vaccinations. Instead of filing vaccine injury cases through the tort system, a specialized federal vaccine injury court handles all cases brought forth by plaintiffs. This court standardizes the litigation process for vaccine injuries to ensure that all plaintiffs have fair and equal trials.
Historical Overview
Vaccination mandates have existed for over three hundred years, with the earliest laws being implemented locally by boards of education, counties, and cities. The first state wide vaccination mandate was enacted in Massachusetts in 1855, requiring all students to be vaccinated against smallpox. Massachusetts had just passed a compulsory school attendance law which drastically increased the number of students receiving education, therefore increasing the risk of smallpox outbreaks. Smallpox is an infectious disease caused by the variola virus, with the more deadly strain variola major having a 30% mortality rate. In 1796, scientist and physician Edward Jenner devised a strategy to protect people from smallpox. Jenner had anecdotally observed that dairymaids were protected from smallpox, and later discovered that it was their exposure to the cowpox virus that protected them. Using cowpox virus inoculations, Jenner created the first vaccine. Despite the existence of a smallpox vaccine, many people were hesitant to use it or did not have access to the vaccine. It’s estimated that over 300 million people died from smallpox in the 20th century alone, well over 100 years after the vaccine’s existence.
The public health benefits of vaccination mandates became increasingly apparent over time, and can be clearly seen when comparing smallpox rates in states with mandates and states without mandates. Between 1919 – 1928, ten states with smallpox vaccination mandates had an average of 6.6 cases per 10,000 people, while six states delegating vaccination mandates to their own localities had 51.3 cases per 10,000 people, twenty-eight states with no vaccination mandate had 66.7 cases per 10,000 people, and four states that prohibited vaccination mandates had 115.2 cases per 10,000 people. In 1971, the CDC recommended discontinuation of the smallpox vaccine from the routine vaccination schedule due to the eradication of the disease in the United States.
The next vaccines were invented in the late nineteenth century, nearly 100 years after Jenner created the smallpox vaccine. The second vaccine to successfully prevent illness in humans was the live-attenuated rabies vaccine in 1885, followed by heat-inactivated typhoid and cholera vaccines in 1896. The smallpox and rabies vaccines produced immunity in the vaccinated individual by exposing them to an attenuated (weakened) version of the pathogen. The heat-inactivated typhoid and cholera vaccines functioned differently, resembling a more crude version of surface proteins and toxins vaccination. By killing the pathogens with heat, the vaccine would not be infectious, but it would still contain the surface proteins and toxins of the pathogen. Over time, scientists further refined these vaccines by producing specific surface proteins and toxins, then measuring them out in more precise concentrations for each vaccine dose. Throughout the early and mid twentieth century, scientists would successfully create many more vaccines, continuously improving their safety and efficacy. After observing the benefits of smallpox vaccination mandates, many states would go on to mandate other vaccines as well.
Introduction
Vaccination mandates in childcare and public educational institutions currently exist for the following 16 pathogens; Bordetella pertussis, Clostridium tetani,Corynebacterium diphtheriae, Haemophilus Influenzae, Hepatitis A, Hepatitis B, Human Papillomavirus, Influenza, Measles, Mumps, Neisseria meningitidis, Poliomyelitis, Rubella, Rotavirus, Streptococcus pneumoniae, and Varicella. To immunize children against all of these diseases, 13 different vaccines are used. Some of these vaccines immunize against multiple diseases. For instance, DTaP provides immunization against Diphtheria, Tetanus, and Pertussis. See Table 1. for the full list of vaccines and the diseases they protect against.
Depending on the ages where protection against a particular disease is most needed, a vaccine may only be required during a specific age range. H. influenzae is a bacterium that can cause severe illness in children under 5 years old, but over the age of 5 risk of serious illness falls dramatically. The Hib vaccine, which immunizes against this bacterium, is therefore only required in children entering daycares and Pre-K education. No states currently mandate that children in K-12 education receive the Hib vaccine, meaning if a child is entering kindergarten and didn’t attend daycare or Pre-K, then they were never legally required to have the vaccine. Booster vaccines are needed if immunity against a disease fades over time. Many vaccines require a series of shots over different periods of time, ranging one month apart (Hep B) to ten years in some cases (Tdap). See Table 2. for the Center for Disease Control’s (CDC) recommended vaccine immunization schedule from birth to 18 years old.
Vaccines included in state vaccination mandates are limited to any one of the thirteen that are listed in the CDC’s recommended immunization schedule for children aged 0-18. Every vaccine listed in the immunization schedule has received a biologics license from the FDA, which means that these vaccines have undergone extensive testing and analysis through clinical trials to ensure that they are both safe and effective. The CDC and state governments receive advice regarding appropriate timing, adequate dosing, and potential contraindications of vaccines from the Advisory Committee on Immunization Practices (ACIP). The ACIP is a panel of fifteen experts independent of the federal government who extensively analyze scientific literature on the topics of vaccines and preventable diseases to formulate vaccination policy recommendations for both adults and children.
Most of the diseases children are immunized against are highly contagious, and can transmit from person to person rapidly in close quarters. Public educational institutions and daycares are examples of such environments where the spread of diseases can occur rapidly, and this is exacerbated in low income areas where schools are often smaller and student to faculty ratios tend to be higher. Contagious diseases each have a value known as an R nought (R0), which represents the average number of people who will contract the disease from a single infected person. Measles normally has an (R0) of 12-18 in most outbreak environments, but in school environments the (R0) can be as high as 40. The best method to combat highly contagious diseases such as measles is through herd immunity. When 85-95% of individuals are vaccinated, transmission rates of that particular disease drop dramatically since a large percentage of people are immune. If 95% of the 12-40 people who’d have normally gotten infected from a measles carrier are vaccinated, then the chances of a full scale outbreak occurring are slim to none.
Although rare, due to abnormal medical conditions, some children are not able to be vaccinated. People with autoimmune diseases or cancer have suppressed immune systems, and they may not have the capacity to effectively develop immunity once vaccinated. Immunocompromised individuals are also at risk of experiencing more severe illness if infected with any of the vaccine preventable diseases. Another serious contraindication to vaccines is anaphylaxis, which occurs when the recipient of a vaccine is allergic to one of its ingredients. People with a history of allergic reactions to vaccines are often advised against vaccinating in the future, unless the ingredient they are allergic to has been identified. With immunocompromised individuals in mind, achieving optimum herd immunity can provide them with an extra barrier of protection against preventable diseases. In an environment with high immunization rates, an immunocompromised person would have to come into direct contact with someone infected to become sick, whereas in an environment with low immunization rates one infected person can spread the disease to other people and indirectly infect the immunocompromised patient. The former scenario is much less likely to occur in an educational setting, and it is generally considered safe for immunocompromised children to attend public schools with high immunization rates.
Current Policies and Challenges
The State and Federal Authority to Mandate Vaccinations
The authority to mandate vaccines arises from police powers that are granted to states under the tenth amendment of the Constitution. Police powers are defined in the Constitution as “the inherent authority of the state (and, through delegation, local government) to enact laws…to protect, preserve, and promote the health, safety, morals, and general welfare of the people. To achieve these communal benefits, the state retains the power to restrict, within federal and state constitutional limits, private interests, [i.e.] personal interests in autonomy, privacy, association, and liberty.” Police powers are exercised by the executive and legislative branches of states through the creation, implementation, and enforcement of laws. Given that several infectious diseases common to the United States are highly contagious and can spread rapidly at educational institutions, public health officials and lawmakers deemed that in order to protect the general welfare of the public, it was necessary to utilize police powers and require students to vaccinate prior to their attendance at public school.
Two constitutional challenges to vaccination mandates were heard by the United States Supreme Court, and in both cases the challenges were rejected after the court determined that states mandating vaccines are permissible exercises of police powers. These cases have since set the precedents to the legal standing of vaccination mandates. The first case, Jacobson v. Commonwealth of Massachusetts, upheld the 1905 state law requiring persons 21 years of age and older to vaccinate against smallpox. The court concluded that the vaccination mandate had a “real and substantial relation to the protection of the public health and safety.” In less than two decades, the Supreme Court heard its second challenge, Zucht v. King, in which plaintiffs argued that the exclusion of their child from school due to their unvaccinated status violated the Equal Protection and Due Process Clauses of the Fourteenth Amendment. The court largely referenced the Jacobson case when rejecting the challenge, concluding that the ordinance did not utilize any “arbitrary power, but only that broad discretion required for the protection of the public health.”
As addressed in the definition of police powers, states can only restrict powers within constitutional limits. In other words, states cannot restrict rights that are protected in the United States constitution. Opponents of vaccination mandates have argued, albeit controversially, that such mandates are violations of their first amendment right, particularly the right to freedom of religious expression. A well crafted version of this argument can be found in the Massachusetts Department of Public Health Memorandum, “the first clause, the Establishment Clause, forbids governments from passing laws that favor any particular religious preference, and the second clause, the Free Exercise Clause, permits individuals to practice their religion freely without interference from government entities. Parents who oppose immunization regulations have argued that requiring a student to submit to immunization that is inconsistent with his or her religious practices is counter to the Free Exercise Clause.” However, with the recent outbreaks in preventable diseases, many states have opted to remove the religious exemption option from their respective vaccination mandate legislation. This move has not been without legal challenges. In 2015, plaintiffs challenged the city of New York for excluding unvaccinated students with religious exemptions during a chickenpox outbreak. The plaintiffs made the following argument: “the statutory vaccination requirement, which is subject to medical and religious exemptions, violates their substantive due process rights, the Free Exercise Clause of the First Amendment, the Equal Protection Clause of the Fourteenth Amendment, the Ninth Amendment, and both state and municipal law. On the same grounds, plaintiffs argued that a state regulation permitting school officials to temporarily exclude from school students who are exempted from the vaccination requirement during an out-break of a vaccine-preventable disease is unconstitutional.” The court ultimately concluded that vaccination mandates are a permissible exercise of state police powers, and they do not infringe on an individual’s first amendment rights.
The federal government has some influence on vaccination mandates, primarily through the Commerce Clause and the Spending Clause of the United States Constitution. “The Commerce Clause grants Congress the power ‘to regulate Commerce with foreign Nations, and among the several States.’ This authority empowers Congress to regulate ‘three broad categories of activities’: (1) ‘channels of interstate commerce,’ like roads and canals; (2) ‘persons or things in interstate commerce,’ and (3) activities that substantially affect interstate commerce. The Spending Clause empowers Congress to tax and spend for the general welfare. Under this authority, Congress may offer federal funds to non-federal entities and prescribe the terms and conditions under which the funds are accepted and used by recipients.” Following the principles of federalism, the federal government can’t require states to pass mandatory vaccination laws. However, the federal government can utilize the Commerce Clause and the Spending Clause to incentivise states to implement vaccination mandates. Such incentives are often provided in the form of federal grants.
Vaccines for Children Program:
A series of measles outbreaks in the U.S. between 1989-1991 sparked a major vaccination campaign to increase immunization coverage. During that period of time there were 55,622 reported cases, approximately 11,000 hospitalizations, and 123 deaths from the outbreaks. The largest outbreaks occurred among minority children in large cities, and constituted up to 82% of cases. Black and Hispanic people represented 17% of the U.S. population at that time, but made up 46% of the confirmed measles cases and 66% of preschool cases in children under 5 years old. Before the large outbreaks, the immunization gap between White children and non-White children was 15%. Following the measles outbreaks, non-White children had a measles vaccination rate of 78% and White children had a vaccination rate of 84%, lowering the vaccination gap to 6%. One causal factor for this immunization gap was the simultaneously present gap in health insurance coverage. The percentage of uninsured White Americans in 1990 was 12%, while the percentage of uninsured Black and Hispanic people was 18% and 28% respectively. At this time, childhood immunizations often required the family to have health insurance, as not every state included childhood immunizations in their Medicaid plans.
To address the large-scale measles outbreaks and immunization gaps between white children and children of color, the Clinton Administration established the Vaccines for Children Program (VFC) in 1994, a vaccination campaign designed to dramatically increase childhood immunizations against vaccine preventable diseases. The goal was to vaccinate over 90% of children against each disease. VFC provided vaccines for children at no cost who were otherwise unable to acquire them, including Medicaid-eligible children, uninsured children, American Indian and Alaskan Native children, and under-insured children (children who have health insurance that doesn’t cover some/all vaccinations). It’s estimated that around 55% of all U.S. children under the age of 19 were eligible for VFC vaccines at the time of its implementation. VFC serves children in all U.S. states, as well as the Commonwealth of Puerto Rico, the U.S. Virgin Islands, American Samoa, Guam, and the Commonwealth of the Northern Mariana Islands. The vaccines covered by the VFC program are ones that protect against the 16 diseases that vaccination mandates address.
The VFC program along with all of the other state vaccination programs and mandates have led to substantial health outcome improvements in the United States. The CDC estimates that the children born in the VFC era (1994-2013) will experience over 322 million fewer illnesses, over 21 million fewer hospitalizations, and nearly 732 thousand fewer deaths from preventable diseases as a direct result of implementing childhood vaccination campaigns and mandates. These estimates do not include influenza (which is included in the VFC) or account for increases in the population, meaning these estimates are artificially low. The VFC program has also closed the immunization gap between white children and children of color over time. For example, the immunization gap was completely eliminated for MMR in 2005, Polio in 2006, and DTaP in 2011. Although the VFC program is expensive, it ends up leading to significant cost savings through preventing doctor visits and hospitalizations. The VFC program is estimated to cost $102 billion in direct costs and $121 billion in social costs, yet it averts an estimated $402 billion in direct costs and $1.5 trillion in social costs. This leads to a net savings of $295 billion in direct costs (hospitalization and treatment) and $1.38 trillion in societal costs (quarantines, loss of time at work, disabilities, etc).
National Childhood Vaccine Injury Act:
Throughout the 1980’s, vaccine hesitancy grew significantly following the publication of “DPT: Vaccine Roulette,” (WRC-TV 1982) a widely publicized television program that depicted children with serious brain injuries thought to be the result of the DPT vaccine. Four viewers of the television program founded Dissatisfied Parents Together, a 501(c)(3) nonprofit organization which has since been renamed the National Vaccine Information Center (NVIC). The NVIC has been long criticized as a leading source of fear mongering, promoting extensively disproven misinformation such as declaring that the MMR vaccine and autism have a causative relationship. Regarding the link between the DPT vaccine and brain damage, investigative journalist Brian Deer provides an excellent analysis in one of his publications, “Brain damage is a catch-all term, and there was nothing to distinguish injuries following vaccination from many of the 2000 causes of brain damage – including genetics, infections, birth problems, and traumas – that often reveal themselves at exactly the age at which DTP is given. In Britain, about 200 babies and infants develop such disorders every week, and by chance 6% will start within seven days of a jab.” Sudden infant death syndrome (SIDS) has also been historically linked with the DPT vaccine. SIDS almost exclusively occurs in infants between the ages of two weeks and one year, a time period in which infants are advised to receive three DPT shots as outlined in the CDC immunization schedule. In the United States, approximately 55 cases of SIDS will occur less than 24 hours after a DPT shot.
Both of the cases described above are based on correlative data, and such data does not prove a causative relationship between the two variables (in this case the vaccine and the suspected side effect). When media sources report on correlative vaccine data, their representation of it can often imply that a causative relationship exists. In the case of “DPT: Vaccine Roulette,” the causative relationship was declared. Extensive studies later demonstrated that the data described in those two cases were correlative and in essence coincidental. Researchers compared the incidences of SIDS between vaccinated and unvaccinated populations, and no relationship between the variables were found in multiple studies. Even though studies extensively disproved a causative link between the DPT vaccine and brain damage/SIDS, the damage had already been done. Trust in vaccines fell, and many parents outright refused to vaccinate their children. Media coverage of the numerous lawsuits against DPT vaccine manufacturers further eroded public trust. By 1987, more than 800 lawsuits were filed against manufacturers of the Pertussis vaccine, totaling more than $21 million. Due to litigation expenses associated with these lawsuits, the Pertussis vaccine rose from $0.17 to $11.00 per dose. One lawsuit settled in the tort system ended with the victim’s family being awarded $1.13 million, which equates to more than half the entire Pertussis vaccine market. The number of companies manufacturing the Pertussis vaccine dropped from 4 to 1, with the last company threatening to abandon production.
The increase in vaccine prices occurred during the Reagan administration, and without immediate action healthcare providers would run out of vaccines to administer to children. To address the rapidly depleting vaccine supply, president Ronald Reagan signed the National Childhood Vaccine Injury Act (NCVIA) into law. The NCVIA was passed to provide a federal no-fault system to compensate vaccine-related injuries and death, eliminating the liability for vaccine manufacturers. Another purpose of the NCVIA was to establish the National Vaccine Injury Compensation Program (VICP). The VICP awards compensation to the families of children who were injured by vaccines, and is funded by a 75 cent excise tax on each vaccine dose sold by manufacturers. The NCVIA led to the creation of a single federal vaccine court system that handles all routine vaccine related injury and death claims. This effectively standardized the vaccine litigation process, preventing personal injury lawyers from filing rampant lawsuits in courts not equipped to properly assess such cases. Similar to civil tort cases, individuals pursuing litigation are required to gather a preponderance of evidence to support their case. However, unlike civil tort cases which utilize expert testimony to support a case, the plaintiffs pursuing vaccine lawsuits must prove that the vaccine caused the injury in one of two methods.
The first method is to prove that the injury in question is one that’s listed in the Vaccine Injury Table, a table which lists potential contraindications that can occur after vaccination. Contraindications that are compensable are added to the Vaccine Injury Table through Department of Health and Human Services regulation in consultation with the Advisory Commission of Childhood Vaccines after extensive research proves the contraindication in question has a causative relationship with the vaccine. Vaccine injuries that are classified as “any idiopathic, unexplained, unknown, hypothetical, or undocumentable injury, illness or condition” are not eligible for compensation according to regulation. The injury in question must also have occurred within a specific time frame following vaccination, and lasted for a minimum of six months (except in the instance of death), or resulted in inpatient hospitalization, or required some form of surgical intervention. The government may counter the plaintiff’s claim if there is any reason to believe that the injury occurred independent of the vaccine. Cases where children develop infantile epilepsy or SIDS following DTP vaccination would be classified as injuries that occur independent of vaccination. See Table 3. the list of vaccines and their respective compensable injuries.
The second method of proving a causal relationship between the vaccine and the injury is pursued when the injury in question is not listed in the vaccine injury table. To prove that a vaccine caused an unlisted injury, the plaintiff must bear the burden of proof through the following three prong tests:
the plaintiff must provide a biological theory of harm,
the plaintiff must provide a logical sequence of events that connect the vaccine to the biological theory of harm in an appropriate time frame,
the plaintiff must rule out any other biologically plausible alternatives to the vaccine(s) in question as causes for the biological theory of harm.
The rationale for the NCVIA and the VICP is to societally compensate for the unavoidable injuries that occur when society mandates that children get vaccinated to attend public schools. Compensation for vaccine injuries are awarded in a lump sum payment and an annuity, ensuring that the plaintiff is compensated for medical costs, estimated lost wages, and pain and suffering. Reasonable legal fees are covered for all plaintiffs who file an injury claim in good faith regardless of the success of their claim. Compensation for death claims are awarded in a lump sum capped at $250,000. Vaccines that are covered in the VICP only include the childhood routine vaccinations for the 16 preventable diseases recommended by the Advisory Committee on Immunization Practices (ACIP). However, a variety of combination vaccines that target the 16 preventable diseases have been in use since 2006, with some still in current use such as the Hep A-Hep B vaccine and others discontinued such as the Hep B-Hib vaccine. Due to the large variety of combination vaccines, more than just the 13 vaccines outlined in the CDC immunization schedule are listed in the VICP’s monthly injury report. See Table 4. for data on the total number doses administered between 2006-2019, the total number of injury and death petitions filed, the total number of petitions awarded, and the total number of petitions dismissed.
Variations in State Vaccination Mandates
By the late 20th century, vaccination mandates for children attending public schools existed in every state and DC. The legality of private schools being exempt from their respective state’s vaccination mandate depends on the particular state. Depending on the state’s statutory scheme, one of the following three scenarios is possible:
private schools and religious schools are exempt,
only religious schools are exempt,
neither private nor religious schools are exempt.
Although some private schools are not required to abide by their state’s vaccination mandates, many still choose to require the same (if not more) vaccinations for their respective students due to the immense public health benefits of herd immunity. Each state decides which vaccines are required, and that number often varies from state to state. Alabama, California, and South Dakota require the least number of vaccines at 7, while Rhode Island requires the most vaccines totaling 13. The average number of required vaccinations among the 50 states and DC is 9, although the exact vaccines that are required vary. Six vaccines are required in every state, and include DTaP (diphtheria, tetanus, and pertussis), Hib, MMR (measles, mumps, and rubella), Polio, Tdap (diphtheria, tetanus, and pertussis booster), and Varicella (chicken pox). Vaccines that are required in half or more states include, Hepatitis A, Hepatitis B, Men ACWY (meningitis), and PCV (pneumococcal virus). Vaccines required in only a few states include HPV (human papillomavirus), Influenza, and Rotavirus. Even if one of the 13 vaccines is not a state requirement where a particular child is located, that child is still eligible to acquire that vaccine free of charge due to the VFC.
Three types of vaccination exemptions are available to students depending on which state they live in.
All fifty states and DC have medical exemptions, which exempt students from vaccinating who have medical conditions that could result in serious contraindications. Such medical conditions include but are not limited to autoimmune conditions, cancer, and allergies to one or more of the vaccine’s ingredients. To acquire a medical exemption, the child must have the application signed off by a physician or other qualified medical authority who deems that the risks of vaccination outweigh the benefits.
Another exemption for vaccinations can be made on religious grounds. If receiving a vaccination goes against a child or their family’s religious beliefs, the family can apply for a religious exemption that waives the vaccination requirements. A religious exemption applies universally to all vaccines, meaning parents can’t use it to exempt their child from receiving certain required vaccines while accepting others. The barriers to acquiring a religious exemption vary from state to state. Some states grant religious exemptions after a few documents are filled out, while other states require proof of membership in a recognized religious organization. As of 2021, 43 states permit religious exemptions.
The last type of exemption offered, albeit less common, is on philosophical grounds. In these states, a parent can avoid vaccinating their children if it goes against their philosophical or personal beliefs. As of May 2021, 18 states permit philosophical exemptions. See Table 5. To identify which vaccines are mandated in each state, and what exemptions are permitted as of May 2021.
By 2000, many preventable diseases had dramatically decreased compared to the years prior to their respective vaccines being licensed. Measles, for example, had 503,282 annual cases on average prior to the existence of its vaccine. In 2000, the number of cases was 81, a 99.98% decrease. Due to vaccination campaigns, wild poliovirus and smallpox have been effectively eradicated in the United States with zero cases occurring during the year 2000. To achieve those decreases in preventable disease rates, many public health interventions were executed across the 50 states and DC. Vaccination mandates for students in public educational institutions played a large role in these decreases in preventable disease rates, as well as federal government action in the form of the Vaccines for Children Program. The vaccination rates of children aged 19 months to 35 months for most diseases during the year 2000 were over 90%, falling short for Polio, Tetanus, and Varicella. With vaccination rates so high and the preventable disease burdens so low, strict enforcement of mandates soon started to fall. The threat that many of these preventable diseases once posed was no longer the same at present day, and the individual risk associated with not vaccinating dropped precipitously. See Table 6. for data on the average rate of preventable diseases three years before vaccine licensure compared to the year 2000. See Table 7. for data on vaccination rates of children aged 19-35 months in the United States during the year 2000.
Even after states had implemented vaccination mandates, a gradual lack of enforcement for non-compliance eventually led to a rise in unvaccinated students significant enough to impact herd immunity. Under state vaccination laws, children who don’t meet the minimum vaccination requirements are to be excluded from attending school. However, enforcement of vaccination mandates varies from state to state. In the 1975/1976 school year, six states implemented stricter enforcement of their vaccination mandates, prohibiting students from entering who weren’t vaccinated and suspending students who did not keep up to date with the required immunization schedule. During the 1977/1978 school year, the six states that had implemented stricter enforcement measures had less than half the rate of measles compared to the rest of the country. The following year (1978/1979) the six states had less than one tenth the rate of measles compared to the rest of the country. Measles outbreaks in Alaska and Los Angeles in 1976 and 1977 respectively led to public health officials strictly enforcing the vaccination requirements. In Alaska, 7418 of 89,109 students (8.3%) were excluded from school due to not meeting vaccination requirements. In Los Angeles, 50,000 of 1,400,000 students (4%) were excluded from school. Within a couple weeks, nearly all of the excluded students were up to date on their vaccinations and back in school. These instances demonstrate that strict enforcement of vaccination mandates are effective, and potentially necessary in some states to meet vaccination coverage goals.
In recent years, social media has propagated vaccine skepticism across the country, leading to a rise in the percentage of children with non-medical vaccine exemptions. The average percentage of kindergarteners with non-medical vaccine exemptions in the 2011/2012 school year was 1.2%. In the 2018/2019 school year, the average percentage of children with vaccine exemptions was 2.2%, with the highest states non-medically exempting 7.7% of children. States that permit philosophical exemptions tend to have a higher percentage of non-medical exempted students. At first glance, these averages may not seem alarming. If 2.2% of children have non medical exemptions, then around 98% of children should still be vaccinated. However, this is not the case. In addition to a rise in non-medical exemptions, states have also recently lapsed in enforcing mandates to non-exempt unvaccinated students. In the 2018/2019 school year, while the average percentage of kindergarteners with exemptions (including medical) was 2.5%, the average number of unvaccinated kindergartners without any exemptions was 2.8%.
When combined, the number of unvaccinated students with and without exemptions has pushed some states below the coverage percentage necessary for herd immunity. This has led to a resurgence in outbreaks of preventable diseases that were once nearly eradicated in the United States. In 2018, 375 cases of measles were confirmed in the United States, usually isolated to small orthodox religious communities. However, in 2019 there were 1,282 cases. This jump in cases was caused by two major outbreaks, the 2019 Pacific Northwest measles outbreak and the 2019 New York measles outbreaks, with both causing their respective states to declare public health state of emergencies. The Pacific Northwest measles outbreak spread throughout the Portland Metropolitan area, with the majority of cases occurring in the Clark County, Washington suburbs. Clark County was known to have widespread anti-vaccination sentiment, and the measles vaccination percentage at the time of the outbreak was just 78%, far below the necessary coverage for herd immunity. By the end of the outbreak, 72 people had been infected. The 2019 New York measles outbreak occurred in New York City and the neighboring Rockland County. The Rockland County suburbs had measles vaccination rates of only 71%, and neighborhoods in Brooklyn with large populations of Orthodox Jews were heavily affected due to low vaccination rates. As a result of the outbreak, the public health officials in Rockland County barred all unvaccinated children from entering school. In response, 42 parents sued the Rockland County health department in an attempt to overturn the order, but ultimately failed when a judge refused to do so. By the end of the outbreak, a total of 649 cases had occurred.
With the recent rise in measles cases, many states have begun removing religious and philosophical exemptions. Following the Disneyland measles outbreak of 147 cases in late 2014, California removed both religious and philosophical exemptions to required vaccines. New York later removed religious and philosophical exemptions following the outbreak in 2019. Other states that have removed non-medical exemptions include Maine in 2019, and Connecticut in 2021. If the number of vaccine exemptions continue to rise, more states will likely remove these exemptions as well. The policy rational states have used for their decisions to remove exemptions stem from the rise in unvaccinated populations, and the costly societal and medical expenses associated with outbreaks. The Washington Department of Health disclosed that over a million dollars was spent to contain the 2019 outbreak. Since the outbreak was a preventable occurrence, significant public outrage followed. See Figure 1 for comparison of what exemptions each state offered in 2014 vs 2021.
Figure 1. Vaccine Exemptions Offered by State 2014 vs 2021
Vaccination Mandates Beyond Public Educational Institutions
Students at public educational institutions are not the only group of people who are required to vaccinate against preventable diseases. Other notable groups who also have to comply with mandated vaccine regimens include healthcare workers, immigrants and refugees, and military personnel. This section will discuss who exactly falls into these groups, which vaccines are required, a brief description of the rationale behind imposing these mandates, and which governing body creates and enforces these mandates.
Healthcare workers who have to vaccinate include physicians, nurses, emergency medical personnel, dental professionals and students, medical and nursing students, laboratory technicians, pharmacists, hospital volunteers, and administrative staff. The CDC recommends that healthcare workers receive the following vaccinations: Hepatitis B, Influenza, Meningococcal, MMR, Tdap, and Varicella. The policy rationale behind requiring healthcare workers to vaccinate is to protect both the workers themselves and their patients. Vaccination mandates for healthcare workers are regulated and enforced by state governments.
Immigrants and refugees who seek residence in the United States are required to show proof of vaccinations before entering. All immigrants and refugees are required to be vaccinated against the following diseases: Diphtheria, Hepatitis A, Hepatitis B, Hib, Influenza, Measles, Meningococcal disease, Mumps, Pertussis, Pneumococcal disease, Polio, Rotavirus, Rubella, Tetanus, and Varicella. The Advisory Committee on Immunization Practices (ACIP), a panel of 15 experts independent of the federal government, provides recommendations to the Centers for Disease Control (CDC) and the Department of Health and Human Services (HHS) regarding which vaccinations should be required for immigrants and refugees. The CDC and HHS ultimately regulate and enforce which vaccinations are required for immigrants and refugees.
Military personnel are required to be compliant with the CDC immunization schedule, and may require vaccinations against other diseases if they are deployed in certain geographic locations. Other diseases that military personnel have to frequently vaccinate against include the following: Malaria, Rabies, Typhoid Fever, and Yellow Fever. Vaccination mandates for military personnel are regulated and enforced by the Department of Defence (DOD). Further, in certain circumstances threats of biological terrorism and warfare may necessitate certain military personell to vaccinate against diseases that are likely to be utilized as biological weapons. The FDA has approved vaccines and antitoxins for the following diseases likely to be utilized as biological weapons: anthrax, botulinum toxin, bubonic/pneumonic plague, and smallpox. Should a novel disease pose a threat to military members, The DOD can seek emergency use authorizations from the FDA to utilize unproven but potentially life saving drugs (including vaccines) to protect military personnel.
Final Reflections: Balancing the Risks and Benefits of Vaccines
Vaccines are neither perfectly safe nor perfectly effective. Inevitably, some people will have adverse reactions to vaccines, and some people will not be adequately protected. From the inception of the VICP in 1988 to July 2021, 24,200 claims of either injury or death were submitted, and 8,162 (approximately 34%) of those claims ended with compensation for the plaintiffs. Different vaccines range in their efficacy, for example the MMR vaccine is 93% effective at one dose and 97% effective at two doses. Despite rare instances of adverse reactions and lack of efficacy, routine childhood vaccines will offer adequate protection and an overall decrease in morbidity and mortality for the vast majority of children who receive them. Over time, all 50 states observed the overwhelming reduction of disease burdens from the implementation of vaccination mandates and followed suit.
One factor that complicates public approval and trust in vaccination mandates is the changes in calculated risk overtime after the implementation of a vaccination mandate. Once a vaccination mandate achieves the adequate percentages for herd immunity, the risk of contracting that disease drops precipitously. Prior to the implementation of the vaccination mandate, the risk of contracting the disease was likely high, therefore the benefits of vaccinating were more obvious. However, once herd immunity is achieved, the risk of contracting the disease lowers, and the risk of adverse reactions to the vaccine are weighed more heavily in the decision making process. This phenomena was apparent in the year 2000 when the United States had the lowest recorded rate of vaccine-preventable diseases in history. During that same year, the United States also had the largest immunization coverage among its domestic population. The preventable disease burden was so low that reports of adverse vaccine reactions appeared in news media more frequently than cases of preventable diseases.
When a disease is nearly eradicated, serious consideration needs to be given on continuing administration of the vaccine if it causes any rare but severe adverse reactions. A good example of this dilemma was deciding whether to administer the oral polio vaccine (OPV) or the inactive polio vaccine (IPV). The OPV offers the strongest protection against polio, and best prevents transmission overall. However, the OPV can cause paralysis. This adverse reaction is rare, occurring at a rate of around 1 in 2.4 million vaccinations. The risk of paralysis from wild poliovirus was much greater prior to the implementation of the vaccine, but over time cases of wild poliovirus dropped. The last instance of paralysis from wild poliovirus occurred in 1979. Every case of paralysis associated with the polio after 1979 occurred as a result of the vaccine. Although eradicated in the western hemisphere, poliovirus still exists in other regions of the world and can easily be reintroduced through international travel if herd immunity is not maintained. The IPV provides immunity against wild poliovirus without the risk of paralysis, albeit not as effectively. In 2000, the United States switched to a vaccine regimen that only utilized IPV due to the risks of OPV outweighing its benefits.
Appendix
Table 1. Vaccines Mandated at Childcare and Public Educational Institutions
Time period for first symptom or manifestation of onset or of significant aggravation after vaccine administration
I. Vaccines containing tetanus toxoid
A. Anaphylaxis
≤4 hours.
B. Brachial Neuritis
2-28 days
C. Shoulder Injury Related to Vaccine Administration
≤48 hours.
D. Vasovagal syncope
≤1 hour.
II. Vaccines containing whole cell pertussis bacteria, extracted or partial cell pertussis bacteria, or specific pertussis antigen(s)
A. Anaphylaxis
≤4 hours.
B. Encephalopathy or encephalitis
≤72 hours.
C. Shoulder Injury Related to Vaccine Administration
≤48 hours.
D. Vasovagal syncope
≤1 hour
III. Vaccines containing measles, mumps, and rubella virus or any of its components
A. Anaphylaxis
≤4 hours
B. Encephalopathy or encephalitis
5-15 days
C. Shoulder Injury Related to Vaccine Administration
≤48 hours.
D. Vasovagal syncope
≤1 hour.
IV. Vaccines containing rubella virus
A. Chronic arthritis
7-42 days
V. Vaccines containing measles virus
A. Thrombocytopenic purpura
7-30 days
B. Vaccine-Strain Measles Viral Disease in an immunodeficient recipient
—Vaccine-strain virus identified
Not applicable.
—If strain determination is not done or if laboratory testing is inconclusive
≤12 months.
VI. Vaccines containing polio live virus
A. Paralytic Polio
—in a non-immunodeficient recipient
≤30 days.
—in an immunodeficient recipient
≤6 months.
—in a vaccine associated community case
Not applicable.
B. Vaccine-Strain Polio Viral Infection
—in a non-immunodeficient recipient
≤30 days.
—in an immunodeficient recipient
≤6 months.
—in a vaccine associated community case
Not applicable.
VII. Vaccines containing polio inactivated virus
A. Anaphylaxis
≤4 hours.
B. Shoulder Injury Related to Vaccine Administration
≤48 hours.
C. Vasovagal syncope
≤1 hour
VIII. Hepatitis B vaccines
A. Anaphylaxis
≤4 hours.
B. Shoulder Injury Related to Vaccine Administration
≤48 hours.
C. Vasovagal syncope
≤1 hour.
IX. Haemophilus influenzae type b (Hib) vaccines
A. Shoulder Injury Related to Vaccine Administration
≤48 hours.
B. Vasovagal syncope
≤1 hour.
X. Varicella vaccines
A. Anaphylaxis
≤4 hours.
B. Disseminated varicella vaccine-strain viral disease
Vaccine-strain virus identified
Not applicable.
—If strain determination is not done or if laboratory testing is inconclusive
7-42 days (not less than 7 days and not more than 42 days).
C. Varicella vaccine-strain viral reactivation
Not applicable.
D. Shoulder Injury Related to Vaccine Administration
≤48 hours.
E. Vasovagal syncope
≤1 hour.
XI. Rotavirus vaccines
A. Intussusception
1-21 days
XII. Pneumococcal conjugate vaccines
A. Shoulder Injury Related to Vaccine Administration
≤48 hours.
B. Vasovagal syncope
≤1 hour.
XIII. Hepatitis A vaccines
A. Shoulder Injury Related to Vaccine Administration
≤48 hours.
B. Vasovagal syncope
≤1 hour.
XIV. Seasonal influenza vaccines
A. Anaphylaxis
≤4 hours.
B. Shoulder Injury Related to Vaccine Administration
≤48 hours.
C. Vasovagal syncope
≤1 hour.
D. Guillain-Barré Syndrome
3-42 days
XV. Meningococcal vaccines
A. Anaphylaxis
≤4 hours
B. Shoulder Injury Related to Vaccine Administration
≤48 hours.
C. Vasovagal syncope
≤1 hour.
XVI. Human papillomavirus (HPV) vaccines
A. Anaphylaxis
≤4 hours.
B. Shoulder Injury Related to Vaccine Administration
≤48 hours.
C. Vasovagal syncope
≤1 hour.
XVII. Any new vaccine recommended by the Centers for Disease Control and Prevention for routine administration to children, after publication by the Secretary of a notice of coverage
A. Shoulder Injury Related to Vaccine Administration
Antibiotic resistance occurs when germs such as bacteria and fungi are no longer as affected by antibiotics. This means that current treatments for various infections will no longer work because the germs that were once vulnerable to antibiotics have adapted to resist them. This can occur when antibiotics are used to destroy some of the bacteria, butthe stronger ones that were able to survive continue to multiply, causing antibiotic resistance to occur.The risk of antibiotic resistance greatly increases when antibiotics are over-prescribed or not used in an effective way.Since overuse allows for the germs to eventually develop resistance to the treatment, areas that lack standard guidelines for treating diseases and prescribing medications are likely to see more infections caused by antibiotic resistant diseases. Healthcare, veterinary, and agriculture industries are also likely to have antibiotic resistant bacteria present due to the higher number of antibiotics used in those settings.
Currently, approximately 700,000 people die per year due to antibiotic-resistant bacteria. According to the World Health Organization, Antimicrobial Resistance (a germ’s ability to resist antibiotics as well as other microbes) isone of the ten greatest public health threatsand will cause an estimated 10 million deaths by 2050. One of the greatest threats are superbugs—bacteria which develops the ability to resist more than one type of antibiotics. Infections that are curable now, such aspneumonia, tuberculosis, blood poisoning, gonorrhea, and foodborne diseases could become impossible to cureas resistant strains spread.
Antibiotic Resistance in the United States
In 2013, the CDC released the first Antibiotic Resistant Threat Report. Since then, different policies have been implemented to reduce the spread of antibiotic resistance. These efforts include Executive Orders issued to direct federal agencies to follow guidelines to combat antibiotic resistance, increased CDC disease monitoring, and FDA directives to ensure that antibiotics are only used for treating and preventing infections in food animals and not for growth promoting. However,there have also been contradicting steps taken, such as the US Department of Agriculture rejecting the WHO’s guidance to limit antibiotic use in livestock feed.
According to the CDC’s 2019 AR Report, the total number of deaths from antibiotic-resistant bacteria fell in the United States by 18% from 2013 to 2019. However, the CDC still estimates there are about 2.8 million infections each year and 35,000 deaths in the United States due to antibiotic-resistant bacteria. Additionally, the number of infections of several strains of bacteria have actually increased, with the germs becoming more resistant and progress to stop infections slowing down. This makes it difficult to find ways to treat those infections and given the interconnectedness of the world, these diseases could then continue to spread. The CDC also estimates that 47 million courses of antibiotics are prescribed each year for cases that do not need it. This is seen in such instances as viral infections like the cold or flu (viruses are not impacted by antibiotics), thereby increasing the prevalence of antibiotic-resistant bacteria as well as allowing already resistant bacteria to develop further difficulties to treatment.
Covid-19 and Antibiotic Resistance
The Covid-19 pandemic has complicated the usage of antibiotics. Antibiotics do not work on viruses, so it would have no impact on Covid-19 treatment. However, since it is possible to get Covid-19 and a bacterial infection at the same time,antibiotics are prescribed to nearly 72% of Covid patients despite only 6.9 percent being reported to have bacterial co-infections. Before there was available widespread Covid-19 testing,it was more common to prescribe antibiotics to patients displaying respiratory symptoms, since it could have been caused by bacterial or fungal pneumonia. Additionally, preemptive antibiotics are often prescribed to stop bacterial infections from occurring at the same time as Covid-19 due to the patient’s weakened immune system. It is important to prevent secondary bacterial infections in Covid-19 patients, though the ratesin which antibiotics are prescribed is higher than the rates of which the bacterial infections occurwith the infections tending to occur in already vulnerable patients. In fact, increases in resistant infections occurred amongst those Covid patients, highlighting how overprescribing antibiotics can create an increase in resistant germs.
Additionally, Covid-19 has generated other obstacles to preventing antibiotic resistance. Due to a shift in focus towards Covid-19, funding has been cut and legislation delayed which would combat antibiotic resistance. Similarly, there may be crisis fatigue in which a loss of motivation arises to tackle another public health crisis. On the other hand, Covid-19 could help set a model for surveillance and containment of other pathogens like antibiotic resistant bacteria. Since antibiotic resistant infections spread very rapidly in hospitals where antibiotics are used, the adopted containment measures from Covid-19 could be beneficially applied towards reducing antibiotic resistant infection spread.Furthermore, the pandemic hashighlighted a lack of surveillance measures among health care infrastructures which creates potential opportunities for surveillance improvements in the future. It is possible that public health approaches learned from Covid-19 could be used to prevent and contain antibiotic resistant infections.
Ways Forward
The CDC has proposed five core actions to reduce the antibiotic resistance threat in the United States:
Prevent and control infections before they arise
Improve data tracking and sharing about diseases
Improve antibiotic use and remove inappropriate access
Increase vaccines, therapeutics, and diagnostics to improve prevention and detection
Prevent antibiotic resistant diseases from entering the environment through sanitation and access to clean water.
There are several ways these goals can be achieved. Increasing funding for agencies responsible for prevention or monitoring of such infections (such as the Food and Drug Administration, the National Institutes of Health, the Biomedical Advanced Research and Development Authority and the U.S. Department of Agriculture) could be beneficial for tasks such as collecting data to track resistant bacteria, improving antibiotic use, and funding antibiotic research. Optimizing current antibiotic use both for human and animal consumption would also help reduce the risks while existing programs that regulateantibiotic distribution could be monitored and directed to ensure the usage of antibiotics is appropriate. Furthermore, developing new antibiotics would help stop antibiotic resistance, since current germs would not have developed resistance towards them. Different bills introduced in congress such as the PASTEUR Actwould create incentives for innovation with different antibiotics. There are a variety of ways in which antibiotic resistance could be combated, and it is important for individuals to consider what methods the government could use to help prepare for such actions.
A vaccine passport is documented proof that someone has received immunization against a specific disease. With the creation of a Covid-19 vaccine, vaccine passports are now being discussed on a local, national, and international level. Vaccine passports have been debated in the United States since the 19th century, when proof of immunization against smallpox (in the form of a scar on the left arm) was required to travel, attend schools, and work certain jobs. Additionally, forms of vaccine passports already exist in the United States, such as students being required to have proof of vaccinations to attend school. According to the Biden Administration, a national vaccine database for Covid-19 is unlikely in the near future. However, different states have differing policies on the issue.
Vaccine Passports on State, Local, and National Levels
New York has established the Excelsior Pass which can be used to track vaccination status and whether someone has tested negative for Covid-19. The Excelsior Pass can be used to gain entry to various businesses and event venues such as theaters, sports stadiums, and wedding receptions It can be used digitally on one’s phone or as a printed paper which documents the individual’s vaccination status. While New York is the first state to implement this technology, other states such as Florida and Arkansas have passed laws which prohibit businesses from requiring proof of vaccination. The EU and Israel have implemented vaccine passports. The EU’s Digital Green Certificate provides documentation of either Covid-19 vaccination or a negative Covid-19 test and allows for members to freely travel throughout the EU. Similarly, Israel’s Green Pass enables those who are vaccinated to enter locations such as hotels and theaters.
Arguments Against Vaccine Passports
One of the biggest concerns when it comes to vaccine passports is individual privacy. Some consider being forced to disclose health information an infringement of privacy. Additionally, the manner in which the data is stored and delivered could raise concerns because there are no standard federal privacy laws regarding the sharing of vaccination status. For example, if vaccine providers such as CVS and Walgreens are not held to the same standards as other medical providers when it comes to handling health information, it can create risks to individual privacy when those companies are delivering individuals’ health information to others. To resolve this,health care entities are working together to develop standards to deliver information while also maintaining individual privacy. New technology could be used to deliver the information without storing individual data, such as CommonPass which communicates with airlines information about vaccinations amongst the travelers without providing private patient data.
Arguments For Vaccine Passports
While some feel uncomfortable with information sharing, others believe the benefits to overall public health outweigh any privacy or liberty drawbacks. In 1905, the Jacobson v. Massachusetts Supreme Court case determined that it was within the rights of the states to mandate vaccination in order to protect public health. At the time, Massachusetts allowed some cities to require laws mandating vaccination against smallpox; however, Jacobson refused to get vaccinated and was fined. The matter was brought to the Supreme Court where it was determined that the states were within their rights to allow vaccination mandates. This is an important component to the Covid-19 vaccine passport discussion since it addresses the question of public health vs personal privacy. Implementing vaccine passports would help to reduce the spread of the disease by creating incentives for individuals to get vaccinated as well as ensure that those who are not vaccinated don’t spread the virus as much.
Other Issues
Another important aspect is equity of vaccine distribution. Lower income communities have less access to the vaccine and receive the vaccination at lower rates. Requiring vaccine passports could further harm those already disenfranchised communities by limiting opportunities that otherwise would have been open. Since the distribution of the vaccinations are not equitable, the impacts of the passports could also fall along similar lines. On an international level, higher income countries are more likely to have implemented vaccine requirements to travel, which further restricts the ability of those from lower income countries to access areas of the world.
Potential Logistics
After receiving the vaccination, there are several different strategies for potential vaccine passport implementation. It is possible for people to either carry the information on a card or store their vaccination records on a digital device such as their phone. Databases, either run by governments or private entities, such as those delivering the vaccines, could also be established to disseminate vaccination information.
Purdue Pharmaceuticals L.P is a private pharmaceutical company founded in 1892 that develops, manufactures, and markets medications and consumer health products. The company has been accused of contributing to the opioid epidemic by aggressively marketing its opioid medications, which are highly addictive. The opioid epidemic refers to the increasing number of deaths and hospitalizations from opioids. Opioids are a type of drug derived from opium, which is a substance from the opium poppy plant. The increased marketing and prescriptions of opioid medications contributed to an uptick of opioid addictions, thus fueling the epidemic. The multiple lawsuits against Purdue Pharma attempt to hold Purdue Pharma accountable for their contributions to the opioid epidemic.
A Brief History of Purdue Pharma
Purdue Pharma was founded in 1892 by John Purdue Gray M.D. and George Frederick Bingham M.D. as the Purdue Frederick Company and was later sold to members of the Sackler family. By 1995, the company was focusing on launching medications that reduced pain. The main product was OxyContin, an opioid meant to relieve chronic pain for those suffering from cancer and other chronic conditions. In efforts to successfully launch the drug, Richard Sackler, the head of the company, hosted dinner programs for physicians who were prescribing greater amounts of OxyContin. The goal became to market the drug to anyone with chronic pain, rather than just those with malignant pain. OxyContin sales reached $48 million. However, the danger of overprescribing powerful pain medications is they are highly addictive. Most who become addicted to opioids do so through prescriptions. Concern grew about the illegal use of OxyContin, as people began to seek out other means to get the drugs, and in the fall of 2000 the problem grew to epidemic proportions. Meanwhile, Purdue Pharma’s sales increased to just under $1.1 billion.
Impacts on the Opioid Epidemic
The opioid epidemic has three main waves – the first starting with drug companies, like Purdue Pharma, encouraging doctors to overprescribe opioids. Doctors told patients that opioids were the answer to chronic pain. However, opioids are one of the most addictive drugs on the market. 21-29% of people prescribed opioids misuse them and continue seeking them out when they are no longer needed. As a result, there were hundreds of thousands of new addictions during the 1990s and 2000s. When doctors give them to patients who don’t require them, it needlessly increases the risk of becoming addicted. The growing opioid addictions brought attention to the problem of overprescribing opioids.
In 2011 there was a crackdown on pill mills, or pain clinics that gave away pills for money, in efforts to decrease prescriptions. As prescription pills became more limited, drug prices rose which led to people seeking street drugs like heroin. The third wave occurred when drug dealers began making synthetic drugs, like fentanyl, that are much smaller and easier to distribute, but are much more potent.
The lawsuits argue that Purdue Pharma played a role in the opioid epidemic when they encouraged overprescribing opioids and engaged in aggressive campaigning that downplayed the risks of using and becoming addicted to opioids. Purdue cited a letter that stated only 2 of 11,000+ patients became addicted when given opioid medicines to validate the safety of OxyContin. In reality, as with most other opioids, it takes a while for the full pain relief effect of OxyContin to settle in. Individuals may look for ways to take the drug quicker to feel the full effects instantly. Additionally, tolerance to the drug builds over time, resulting in the person needing more and more of it to experience the same effects. This is how addictions begin and this is what Purdue Pharma downplayed when marketing the drug. In fact, Purdue Pharma spent more than $400 million in promotional spending. This aggressive campaigning helped spread the word, increase the sale of, and claim the false safety of OxyContin.
The Lawsuits
2002 – Florida attorney general’s office was one of the first law agencies to investigate Purdue Pharma. It cited almost 400 pill deaths in three Florida counties in the past 2 years and claimed Purdue Pharma was the one responsible.
Contributing a total of $4.5 billion to charities aimed at ending the opioid epidemic. These funds will come from both the Purdue Pharma company and the Sackler family’s individual funds.
This case is the highest profile case against drug makers, pharmacies, and distribution companies, which are the main producers of opioids. However, the Sackler Family didn’t actually admit to any wrongdoing. The settlement doesn’t hold the family accountable and they’ll continue to be one of the richest families in the US. Furthermore, some attorneys argue that the settlement gives the Sackler family immunity through Purdue’s bankruptcy. In addition, the harm caused by the opioid epidemic is vast and while holding a major pharmaceutical company accountable is a step in the right direction, it won’t reverse the costs of the epidemic.
There were more overdose deaths in 2020 during the pandemic than any other year, reaching nearly 100,000 deaths. Every day around 128 people die from an opioid-related overdose. One problem that has persisted when trying to address the opioid epidemic is cutting supply, rather than focusing on reducing the demand. As a result, people resort to other more dangerous means, making that solution inadvertently further the epidemic. Perhaps more focus should be on drugs like buprenorphine and methadone, which help reduce the overdose death rate by 50% or more. In addition, naloxone, the life-saving medication that can prevent deaths from overdoses, should be widely distributed. More recovery centers, mental health resources, and training to administer life-saving medications are also needed to help combat the opioid epidemic, along with holding large pharmaceutical companies accountable.